January…February…March…April…May…June…July…August…September…2020 here
This is a chronology not based on the date the information was published but based on the date I decided to publish it.
Those who accuse this site of hyperbole would have thought that even suggesting the possibility of half of what’s happening today just over a year ago was hyperbolic and paranoid. The sleep of subversive reason is spawning an epidemic of monsters.
It should be clear that I am not in accord with the ideological aspects of the content of many of the articles I link to. And, as with all information about Covid, articles have to be filtered through a critical vigilance that I personally have sometimes not invariably exercised in relation to various articles, at least at the time of putting them up. I put them up because they seem to offer alternative sober perspectives on what’s happening.
I should also add that there may well be some inconsistency and contradictory information here. That’s because it’s extremely difficult to sift what is valid, what is speculation and what is manipulation. However, it seems more worthwhile trying to put forward some of what appears to be the more pertinent criticisms of what’s going on than remain silent before the overwhelming propaganda machine and wait a few years in order to be “correct” but too late. “The path toward simplicity is the most complex of all, and here in particular it seemed best not to tear away from the commonplace the tangle of roots which enable us to transplant it into another region, where we can cultivate it to our own profit. ” – here
31/10/21:
Chomsky calls for apartheid and potential starvation of the non-vaccinated
See also this, from a few years ago, about this deeply hypocritical “critic”. To summarise the most significant bits – he defended another fellow academic, Walt Rostow, and his freedom of speech even though, as a government adviser, he had organised the US’s murderous bombing of North Vietnam and then, in 1969, threatened to ‘protest publicly’ if Rostow were prevented from returning to his academic job at MIT. He also defended the freedom of another MIT academic, John Deutch, to research whatever he wanted (even if he did research the use of ‘chemical and biological weapons together in order to increase their killing efficiency’ as well as initiating the deployment of both MX and Midgetman nuclear missiles) and was ‘one of the very few people on the faculty’ who supported Deutch’s bid to become MIT President. He also supported, in The New York Times, Deutch’s promotion from Pentagon official to the Director of the CIA in 1995. In 1969, Chomsky openly told anti-war students that, rather than trying to remove war research from the university, ‘you ought to have the Department of Chemical and Biological Warfare right in the centre of the campus so you can see who is coming and going.’ It helps us understand why, at this time, Chomsky opposed students’ attempts to occupy MIT’s administrative offices in protest at their university’s military research. See these for more details:
‘Chomsky at MIT: Between the war scientists and the anti-war students.’
‘John Deutch – Chomsky’s friend in the Pentagon and the CIA.’
Germany: some Deepl-translated extracts from the transcript of a fairly rambling German anarchist podcast about the past and present of Covid1984 there
“…Overall, a value-critical, labour-criticising movement has largely been steered into harmless channels and has largely welcomed the lockdown. Marxist theory as a whole has actually nothing to oppose the current oppression and lockdown. For those who see only exploitation and not domination (not to speak of technology) see only half of the problem…
It is true that initially many took advantage of the situation to skip work & co. It is intelligent that this moment, which was not actually calculated in this way and was initially rather opposed to the normal administration of the population, is now being appropriated. It is necessary to understand how far the subversive content of certain gestures has been emptied and to what extent these refusals were so subversive in the first place, at least since all the Corona strikers were largely taken in by their own excuses and have now become entangled in them. It has at least now become obvious that these refusals must rather be understood as an entry into the promised land of VR. The technological universe that is now supposed to replace normal direct human exchange is thus getting a boost, although technology is the initiating force anyway. It causes the inward spiral, an addictive dynamic, which everyone is actually aware of…
The technological process also has a subversive effect, but only in order to stabilise and advance itself. Any insurrectionary and revolutionary subversion must therefore first avoid being steered in such directions. For these mean stemming the tide, or rather ushering it into the maelstrom of technology, which is ultimately productive. Productive for the world of technology and capital. As promising more control. Since more information. And this making oneself into information is precisely the new work, even if it is gamified. Or even not only gamified, but effectively seems to be a game.
It’s difficult to discern one’s own relationship to this reality. It is clear that one is not outside. It is clear that refusing to work only leads to a new misery, if one does not try to destroy work. The world of work. This world that is completely built on work. That is: not to work. That means: to revolt against one’s own role. And this role is now also the role of the “lazy sod” (sic!) who sits at home and plays games. Because power has understood more and more that every role and identity can be used. That none of them is actually dangerous as long as it can be identified and built into the spectacle.
And the mass-mobilising spectacle that is taking place has all too suitable roles at the ready. For example, the conspiracy theorist (occasionally also aka. anti-vaccinationist aka. gadfly etc.), who is allowed to stand as a scarecrow in front of any criticism. A scarecrow that would have to be invented if it did not exist. Thus any form of reference to certain facts can be contaminated with it (such as Event 201, or Pandemic Level 6, or Swine Flu, or Bill Gates’ rupturist “World Health Imperialism”, or id2020). Whereby this helps the QAnon movement in the best possible way. While the granny next door is now hoping that Trump will free us from the lockdown. Divide and conquer, yes yes.…
Clearly, one can criticise the lockdown without saying a word about Bill & Melinda Gates Foundation, the history of WHO, Rockefeller Foundation and Gavi, for example. That has been done enough. It is equally clear that it is a dead end to simply dump on Gates & Co. But it is the logical development, given the fact that the hypnosis by “Corona, Corona, Corona…” is simply replaced by “Gates, Gates, Gates…”. Those who now make a Corona Committee, etc., they react from their perspective, and for them the specific responsible persons are also logically extremely important. After all, they want to hold them legally responsible. Perhaps also lynch them. All this is understandable, and why not? But it remains in the dimension of a political spectacle. The viewer is not swept off his feet. He remains a spectator or even becomes an active supporter, takes to the streets… but the fundamental question, which is exciting for us, is not touched.
And then of course the anti-fascist spectator. He sees the Nazis crawling out of their holes, and already everything that opposes these Nazis (if at all) becomes a friend. One’s own lack of perspective and criticism does not allow one to understand that one has actually been enforcing conformism for a long time and fighting deviation from the social norm. It is not wrong, loosely based on Adorno, to call the people of Querdenken & Co. “”conformist rebels” who rise up against “the system” and yet want everything to remain as it is”, as the initiative “Enlightenment instead of Conspiracy Ideologies!” does. But just as Adorno’s critique is made ridiculous by the fact that he called the cops on the students who occupied his institute, this critique is also depriving itself of ground, since one seems to want to outdo the lateral thinkers [Querdenken means “lateral thinking” – SF] not in rebellion but in conformism…
But anyway: in postfacticism, facts and assumptions are tied to identities and roles. And so everything is contaminated (not only with Corona (-;). And while one reality belongs to one party, other facts etc. belong to the other. And so it is administered, can be administered best. And almost nobody does their own analysis any more anyway.
And in the end, it’s all people doing their business. Defending their interests. Or want to mobilise you. From Ken Jebsen to Korrektiv, from Bill Gates to Trump, from Söder to Bolsonaros, from social democracy to QAnon, from Widerstand2020 to the Rosa Luxemburg Foundation, from left to right, across the centre… from Drosten to the Corona Committee… yes: from Querdenken to Antifa… all of them will not liberate you and will not protect you. They want to make capital out of you, be it ideological or political capital. They want to manage this society, in one way or another. Defend its foundations. They represent no other horizon than the one that reduces you to a spectator or a cog or burns you as cannon fodder, alone at home or back at work… blocking the possibility of real liberation…
Ever since the Bavarian Office for the Protection of the Constitution noted in bewilderment that the “left-wing extremists” had apparently become loyal to the government in the “Corona crisis” (which is true), it seems to me that not too much really needs to be said about the left any more. Such praise actually says it all. Likewise, with Zerocovid, the left scene has also finally started to split. We say: that’s good! but, dear (alleged) revolutionaries: one more effort if you want anarchy! Because as long as you want to re-breathe the carcass of the left, you will only ever breed new authorities and new compromises, you will (re-)produce a movement that will lead you to one dead end or another instead of to social revolution….
while the right today complains (amusingly, one might say, if things weren’t so serious) that they are now all treated like refugees, when it was they who enabled the state to train for today’s lockdown reality on refugees… the left has moved on to being satisfied with everyone being treated like refugees – at least then no one is discriminated against. “Great, finally everyone has no more privileges!” And so the left fights those who again want the “privilege” of not being completely patronised, controlled, harassed, etc., instead of criticising them for wanting the same as a privilege, while they don’t find paternalism, control and harassment so bad in others. And consequently, the left wants to oppress the right and the right wants to oppress the left. Or: both want their form of oppression.
A world without borders, without fatherlands, without property and the rich, without statisticians and experts, aparratschiks and block wardens, a world without police and without cybernetics, without bureaucracy and speculation, without paternalism, control and harassment… such a world we carry in our hearts when we fight, with such an idea we plunge into the social conflict, and there leftists as well as rightists as well as centrists are our enemies, although the small risk is interesting that we nevertheless meet as individuals who self-determinedly rebel against their oppression and leave politics behind them…. while in the past the assumption was that such people would be found mainly among leftists, today it has to be said that humanly they are now often just as disgusting and low as any open reactionaries and racists, with whom there can of course be no common ground…”
30/10/21:
Israeli physicians, scientists advise FDA of ‘severe concerns’ regarding reliability and legality of official Israeli COVID vaccine data
Lists the following problems:
Lack of a Public and Transparent Adverse Events Reporting System, Severe Impairments in Healthcare Professionals’ Adverse Events Reporting System, Data Distortion, the deletion of thousands of citizens’ responses, Legal and Ethical Violations in Data Collection Processes.
Doubtless all this will be ignored, or dismissed as conspiracy theory. The immeasurable deterioration in the rational desire to try to understand what’s going on, significantly exacerbated by the intensification of isolation brought about by the increasing destruction of working class communities, is resulting in capital’s global capacity to make the vast majority to dance to any tune it seeks to play them.
29/10/21:
Some recent statistics which seem to be valid (though not 100% sure) regarding infections of the under 50s in the UK:
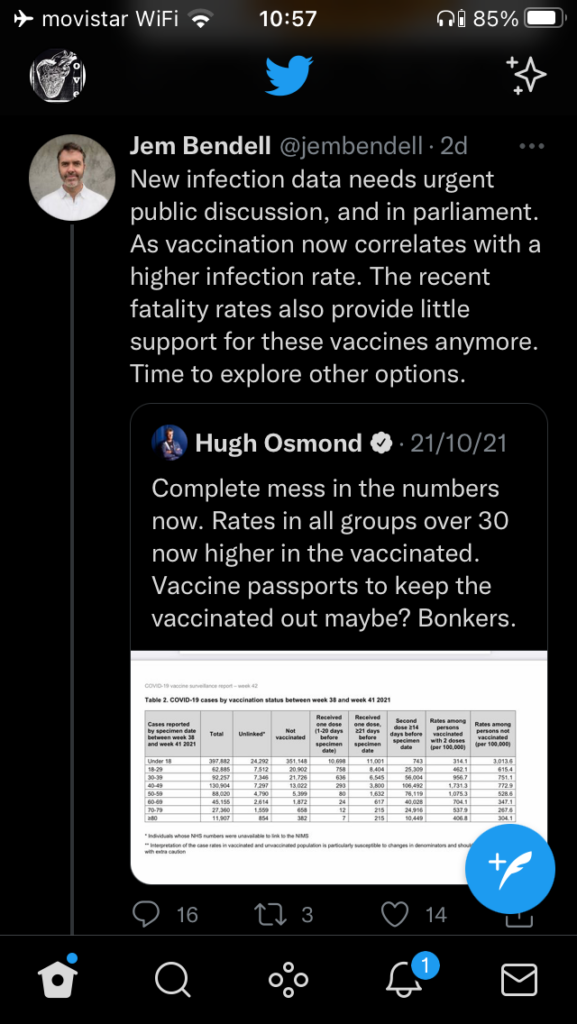
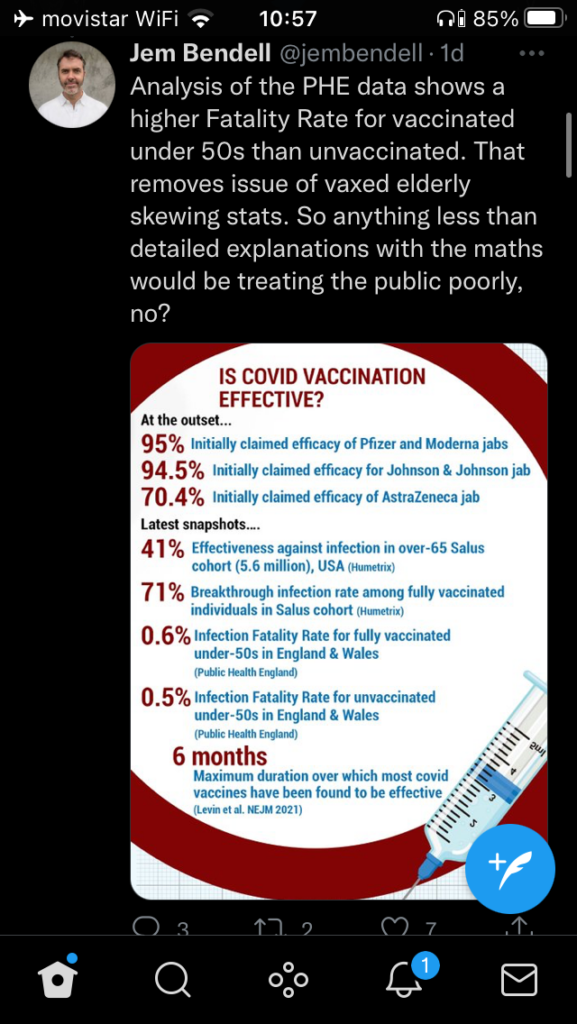
Case fatality and severe illness for those over 50 is significantly reduced for those who’ve been vaccinated, so it would be useful as a voluntary tool for people at high risk. But as far as the UK data demonstrates, it is worse than useless at “stopping covid”, which has been the justification for all the hype and repressive measures to date.
28/10/21:
Deepl translation of part of this (much of this, including the rest of this longish text, is passionately written but not sufficiently nuanced):
“…What does genetics actually do all day long when it is not concocting grand plans to treat the whole of humanity with its poisons? Locked up in their laboratories, the ladies and gentlemen of genetics are on the trail of something great day after day: the secret of life. But it is not life as you or I might understand it. Life, for the geneticists, consists of cells. So when geneticists claim to decode human life, it means that they – at least theoretically – cut a human being into tiny little pieces, put them in Petri dishes and then look at these cadaveric remains through a microscope. Because these particles reproduce themselves in a Petri dish under certain conditions, they call it the basic building block of life. Except perhaps for the scientists themselves, everyone now understands that this is not human life, but if anything, it is death artificially brought to life. And to avoid the insult that every layman understands more about life than they do, the geneticists consequently occupy themselves with creating artificial life in their laboratories, life that consists of those basic building blocks of living death, called cells, and which the confused layman, who may still wonder at the feat of transforming something dead into something that looks so alive at first glance, now actually believes to be life. The geneticists, on the other hand, most of them true Christians, henceforth feel godlike. For apart from them, as is reported in a well-known myth, only God has so far succeeded in breathing life into dead matter. In their delusions of grandeur, they too overlook what the layman had to overlook because of his amazement: they have not created life, but merely a new kind of machine. Some people therefore call genetics – and not only genetics – necroscience, i.e. the science of death.
In the meantime, however, we are faced with the very real problem that the life that geneticists have mutilated in their laboratories no longer always dies miserably on the experimental table, but escapes from these laboratories from time to time or is released into the wild by the geneticists themselves. Genetically modified plants and animals – and recently even humans – walk outside the laboratories of their tormentors and we can no longer regard them as the living dead, but at best as life mutilated by their creators. And let’s be clear: Only an idiot would take advantage of Frankenstein’s monster. Anyone in their right mind kills Frankenstein!…”
26/10/21:
UK: Interventions against vaccinations in schools against vaccinations for 12-18-year-olds
This, of course, is a mainstream pro-vax report (includes a description of these interventions as “Trumpian” without any attempt to justify such an amalgam technique). So somewhat biased. Perhaps some aspects of the tactics are dubious, but considering that a lot more kids die annually of flu than of Covid, some form of intervention seems vital: people of this age are hardly threatened at all by Covid.
23/10/21:
Child deaths significantly higher since vaccine
Hard to know what to make of this as it’s put in rather vague terms. But I put it here for the record.
21/10/21:
Italy, Trieste: report on clashes following cop attack on dockers’ blockade of port in protest against Health Pass
“While the dockers of Trieste have been blocking the port for several days, the police have intervened to evacuate the opponents of the sanitary pass with water cannons. Trieste alone has more protesters than Rome or Milan. The dockers who have been blocking the port of Trieste for three days to oppose the health pass in Italy were confronted by the police during an intervention on the morning of 18th October. …Stefano Puzzer, head of the CLPT (the workers’ committee of the port of Trieste), had however assured that the action would not hinder “those who want to work”, leaving the port to operate in slow motion. The union had also announced an extension of the strike: “We don’t accept the proposal of free tests, we defend our free will”, said Stefano Puzzer on the subject of the vaccination and the health pass, which are compulsory to go to work. However, police vehicles arrived in front of Gate 4, from inside the port, as reported by the ANSA news agency. Protesters waited for them on the other side of the gate, along the road, sitting on the ground chanting “people like us never give up” and “freedom”. The police were equipped with riot gear, and an official repeatedly told them to disperse “in the name of the law” before resorting to water cannon. …When the water cannons stopped firing, the demonstrators resumed their sit-in, slowing down the intervention of the police vehicles. Meanwhile, more people arrived in the square – mainly in support of the protesters – where there were already about a thousand people, according to ANSA. Port workers, recognisable by their yellow waistcoats, had formed a cordon between the police and the demonstrators to avoid clashes. The police nevertheless ended up charging the dockworkers to unblock the port while resorting again to water cannons but also to tear gas. Located in Istria, on the Slovenian border with Italy, Trieste has become the epicentre of the protest against the Green pass. On 9 October, more than 15,000 demonstrators gathered before port workers began a blockade on 15 October.”
More developed radical report on situation in Trieste and the rest of Italy here
“…While the political climate continues to polarize, with the regime media not sparing the opportunity to accuse the entire movement of being led by the fascists, and made up of individualists, deniers and conspiracy theorists, in Trieste a growing part, albeit a minority of comrades, tries to channel the anger against the Green Pass. Here too, in the fight against the green passport, very heterogeneous people are mixed together, both in terms of social class and in terms of the beliefs that lead them to express their dissent. Nevertheless, the Coordination, together with the dock workers, decides to stay within the movement, aware of its ambivalence.
The comrades decide to stay in the assemblies starting from the assumption that every mass movement always contains within itself positions that are often very different, in some cases apparently irreconcilable, without it being necessary to marry them all. It is in the assemblies that the most advanced currents can prevail, to oppose all forms of blackmail and discrimination in the workplace, as well as in social spaces, to oppose increasingly invasive forms of biopolitical control and the limitless expansion of the State of Emergency, to counter the capitalist management of vaccination programs, to avoid transforming science into a dogma, as when the usefulness of the third dose is criticized by a fairly large part of the scientific community…”
And more on Italy
Ivermectin in early treatment in Australia
Physician and researcher Thomas Borody, reports on an outpatient Ivermectin-Doxycycline-Zinc triple therapy treatment experiment involving 600 patients, with an untreated, voluntary, control group (randomized).
This study is an observational study, from June to September 2021, stopped at 600 patients, following the prohibition of general practitioners to prescribe Ivermectin by the Australian authorities (TGA). Results collated from over 30 doctors, in two states. A publication is in preparation.
The 10-day treatment: Ivermectin at a consistent dose 24 mg/day, Doxycycline 100mg/day, Zinc 50 mg/day. All patients were treated within 48 hours after a positive PCR test. None had to stop due to side effects. In the treated group, 5 hospitalized (0.78%), 0 deaths. In the control group, 70 hospitalizations (11.5%) and 6 deaths (1%), figures that are consistent and found everywhere.
A subgroup of 126 people (17 to 92 years old) was quarantined (in a hotel or at home) and followed more closely on 10 criteria. All oximeters normalized within 10 days, the most persistent symptoms were loss of taste and smell.
Borody compared his groups with those in the Merck study (385 patients) of Moneypiravenir. The placebo groups in both studies had the same rate of hospitalizations and deaths. However, in the group treated with its antiviral, Merck had 8 times more hospitalizations.
The results of this study are quite consistent with those found in the vast majority of the 63 published studies on Ivermectin, carried out in 20 countries by 625 authors and involving 47,500 patients.
A similar study with more cases could be done in France with the evidence we have, but the doctors have to hide themselves from it. How embarrassing would it be if it were done in full transparency, controllable by the patients? Apparently, those who forbid it are afraid of the result of such a study and its impact.
It has been decided by the ANSM [Agence nationale de sécurité du médicament et des produits de santé] that Ivermectin “has strictly no action, either as prophylaxis or in therapy”. This decision (a decision, not a finding) is not medical, but political and financial. Moreover, they refuse to give us the conditions of this decision, even though the law requires it.
Who is then Thomas Borody who was able to do this in Australia, in a health dictatorship that is as good as ours? Not known in our country, and yet! In Australia, this doctor and researcher is very well known and respected. It is also true that since the arrival of covid, those who were experienced and well known (cf Didier Raoult) have been discredited in favour of statisticians and modellers who are not medical doctors. Decisions that cannot be explained medically are then taken within the framework of a security secret.
Borody is somewhat in this situation in Australia, but what is surprising is that this is the second time in his career. He led the fight for antibiotic therapy in stomach ulcers (reported on in this blog), taking over from Barry Marshall and Robin Warren who had discovered Helicobacter pylori, to set up a protocol that now means that stomach ulcers are no longer operated on, that cancers have decreased, and that hundreds of thousands of lives have been saved. This is the second time he has defended a Nobel Prize-winning treatment. He knows what he is talking about because of his experience with stomach ulcers, and also because he has since devoted his career to the study of intestinal bacteria and has pioneered antibiotic therapies for a whole range of conditions not explicitly associated with bacteria.
Indeed, at the time, treating ulcers with antibiotics was nonsense, as was treating the flu with antibiotics. Advocates of this treatment were ridiculed by their peers, summoned by the Order of Doctors, scorned by the president of the Gastroenterology Society, and banned from publication. 20 years of fighting against skeptical and septic scientists, influenced at the time by the laboratories selling antacids (anti-ulcer drugs were among the best-selling drugs in the world), until Marshall and Warren were awarded a Nobel Prize in 2005. Borody hopes it won’t take 20 years to win as it did for Helicobacter, and he points out that at the time, “the most educated levels of society are the most difficult to change their views. There is a flat-earth mentality.” We are at the same point with ivermectin, preconceived and false ideas, which some people do not want to change.
How Ivermectin became a Target for the ‘Fraud Detectives’
19/10/21:
Deepl translation of this critique of the health pass situated in its historical context:
“Critics of the health pass unanimously denounce an “authoritarian danger”. Quite rightly, the CNIL itself presents this danger as “the risk of habituation and trivialisation of such privacy-invasive devices and of a shift, in the future, and potentially for other reasons, towards a society where such controls would become the norm and not the exception”. Let’s take a moment to detail this danger and answer the question: what kind of surveillance is the health pass?
There are already many “privacy-invasive devices” that we have been fighting against for years: phone tapping, data filing, cameras, drones, geolocation, spyware, etc. To understand and prevent the dangers posed by the security pass, we need to situate it precisely within this ecosystem. Some surveillance tools are more or less easy to deploy, on a larger or smaller scale, in a more or less visible way and with very variable consequences. By understanding the technological movement and the pre-existing tools the health pass has been built upon, we hope to fight more effectively against the trivialisation of the type of surveillance it allows.
Controlling to exclude
To take a step back, let us describe in general terms the action that the health pass makes possible: to exclude from certain jobs, transport and places people whose situation differs from certain criteria set by the State.
Formulated in this way, there is nothing new about this method of regulation. This is how the French state treats foreigners: access to transport to the national territory, and then access to residence and employment on that territory, is only allowed if the situation of the foreigners complies with criteria set by the state (personal family and economic situation, country of origin, age, etc.). Compliance with the criteria is first checked beforehand and is then reflected in the issue of a document: visa, residence permit, etc. Then, the police only have to check the possession of these documents in order to control the situation of the persons, and then open or close the corresponding accesses. By threatening to exclude people who do not have the right document from the territory or from employment, the state deploys heavy repression – the consequences for those excluded are particularly dissuasive.
However, until recently, this type of repression had important practical limitations: documents could only be issued with a certain delay and at a certain cost, many police officers had to be deployed to check them, and some police officers even had to be specifically trained to check their authenticity. These limitations probably explain in part why this type of repression has so far been focused on specific cases (such as the control of foreigners) without being systematically deployed to deal with any situation that the State might wish to regulate.
The health pass is the translation of technical developments that could remove these old limitations and allow this form of repression to be applied to the whole population, for a very wide variety of places and activities.
Scaling up technology
Over the last decade, the majority of the French population (84% in 2020) has acquired a smartphone equipped with a camera and capable of reading 2D barcodes, such as QR codes. At the same time, the administration has largely adopted the tools of 2D barcodes and cryptography in order to secure the documents it issues: tax notices, electronic identity cards, etc. The 2D code makes the cost and speed of writing and reading information on a paper or digital medium almost zero, and cryptography makes it possible to ensure the integrity and authenticity of this information (guaranteeing that it has not been modified and that it has been produced by the authorised authority).
Although these developments are not particularly impressive in themselves, their concomitance makes things possible today that were unthinkable just a few years ago. In particular, it makes it possible to entrust tens of thousands of untrained and unpaid people from the state (but simply with a smartphone) with the task of checking the entire population at the entrance to countless public places, and this at an extremely low cost to the state since the bulk of the infrastructure (the phones) has already been privately financed by the people in charge of the check.
Now, suddenly, the state has the material means to regulate public space to almost total proportions.
One more brick in the Technopolice
The health crisis has certainly facilitated these developments, but its role should not be exaggerated. This dramatic increase in the powers of the state is part of an overall movement that has already been at work for several years, which did not wait for the coronavirus, and against which we are fighting under the name of ‘Technopolice’. It is the deployment of new technologies aimed at transforming cities into ‘safe cities’ capable of regulating the entire public space.
The Technopolice is the expression of technological developments which, as we have seen with the case of the health pass, have made it possible to make total forms of regulation which, until then, were more or less targeted. Let us take the emblematic case of cameras: until recently, the police were materially limited to a targeted video surveillance policy. They could only use the video recordings to analyse a few targeted situations, as they could not put an officer behind each camera 24 hours a day. Similarly, the identification of a person filmed required significant effort.
These limitations have since been overcome. Facial recognition makes it almost trivial to identify the people filmed (see our presentation). Automated image analysis makes it possible to continuously detect all events defined as “abnormal”: panhandling, being too static, running, forming a large group of people, drawing on a wall, etc. (see, for example, the projects imagined in Marseille or Valenciennes). It is no longer necessary to place an agent behind each camera to have a total vision. Whether it is the health pass or automated image analysis, in both cases technology has allowed targeted techniques to be transformed into tools for mass control of public space.
Permanent control of bodies
This parallel allows us to make an important clarification: whether it is the health pass or the automatic detection of ‘abnormal’ behaviour, these systems do not necessarily require an identity check. The imaging software that reports your “abnormal” behaviour doesn’t care what your name is. Similarly, in theory, the health pass could also work without your name – this is what the original crisis exit legislation envisaged or, more worryingly, what some companies are now proposing based not on name but on face. In these situations, all the state cares about is directing our bodies in space in order to send to the margins those who – no matter what their names – do not conform to its demands.
This control of bodies is done continuously and at all levels. Firstly, to detect bodies deemed ‘abnormal’, whether by their behaviour, their appearance, their face, their vaccination status, their age… Secondly, to constrain bodies and exclude them from society, whether by the armed force of the police or by bans on entry. Finally, to inhabit bodies and minds by making us internalise the rules dictated by the state and by pushing people who do not submit to them into self-exclusion. All this on a population-wide scale.
Unjustified addiction
The mass adoption of the health pass would have the effect of accustoming the population to submit to this mass control, which is part of the broader cultural battle already initiated by the government, notably around cameras. This habituation would make it easier for the state to pursue its total conquest of public space, as it has already begun with the Technopolice.
Yet, paradoxically, in its current format, the health pass does not appear to be a very effective regulatory tool itself. It seems difficult to prevent doctors who wish to do so from providing passes to people who should not receive them. And, even if the passes are given to the “right people”, as it stands they can easily share them with the “wrong people”. Of course, the police intend to carry out identity checks to combat these exchanges, but if the effectiveness of the system ultimately relies on random police checks, there was no need to deploy mass surveillance mechanisms to go beyond what is already being done in this area, for example with handwritten prescriptions issued by doctors, which the police can check if they are suspicious. This would at least reduce the risk of addiction to a new system of mass surveillance.
Unfortunately, it seems more serious to envisage the opposite scenario: the ineffectiveness of the health pass could be used as a pretext to perfect it, in particular by allowing non-police controllers to detect pass exchanges. As seen above, some people are already proposing a new system displaying the face of the people being checked. Such a development would deliver the fully developed and effective version of the mass control system dreamed by Technopolice – and the police would hardly have to work at all to control passes.
Requirement to prove necessity
Even in its most sophisticated format, the health effectiveness of the pass would still need to be demonstrated – there are many uncertainties, whether about the value of the tests after 72 hours, the rate of transmission even after vaccination, the case of new variants, the effectiveness of coercion in getting people to vaccinate, or the length of time that the screening tests should be valid.
From a legal and political point of view, and as we recalled for StopCovid, the State is subject to a simple but fundamental rule: it has the obligation to prove that a measure causing risks to fundamental freedoms is absolutely necessary before deploying it. In our case, not only has the government not yet demonstrated the effectiveness of the health pass but, more seriously, it has refused to deploy or test the effectiveness of alternative measures that would not cause any risk to freedoms (such as benevolent, transparent and non-paternalistic communication campaigns to invite people to be vaccinated*), or ambitious complementary measures (such as the release of funds to allow the doubling of classrooms and their ventilation, which the government has simply ruled out).
Conclusion
To summarise: the health pass illustrates technological developments that allow an old mode of repression (repression through exclusion, illustrated in particular by the control of foreigners) to move from a relatively restricted scale to an almost total scale, concerning the whole population and public space, in order to send back to its margins those who do not submit to the injunctions of the state.
If, today, these injunctions are only of a health nature, we must once again fear that this type of tool, once it has become commonplace, will be used to serve injunctions that go far beyond this framework. This fear is all the more serious because this process has already begun within the Technopolice, which is already sketching out a mode of social regulation based on the detection and exclusion of anyone considered deviant or ‘abnormal’ in the eyes of the state and the security companies, which together define the new norms of behaviour in society in an opaque manner.
A final strategic reminder: one of the reasons why the French government allows itself to impose such tools for the detection and exclusion of people it deems undesirable is that it can take up, and in turn revitalise, the obsessions that the far right has managed to trivialise in public debate in recent years in order to track down, control and exclude a certain section of the population. The fight against the authoritarian risks of the health pass would be futile if it were not accompanied by a fight against the extreme right-wing ideas that were its beginnings. The fight against the health pass must not be done with, but against the extreme right and its obsessions, whether they are in the street or in government.”
*SF note:
This is a dubious statement to say the least: given that these are essentially experimental vaccines and that the state has already misinformed people of many aspects of it, “non-paternalistic communication campaigns” is just a nice phrase without any possible realistic meaning.
18/10/21:
Against Vaccine Passports
France, Martinique (overseas territory): clashes outside hospital as hospital workers demonstrate against compulsory vaccination (16th Oct.)
“Carers trying to storm the hospital, repelled by CRS. A few minutes earlier, two of their comrades were handcuffed on the ground. They were arrested after throwing projectiles at the police….In the courtyard of the hospital, scenes of rare violence. Everything that can be used as a projectile, benches, blocks, is thrown, including from the upper storeys. In the images, we can also see the flag of the Martinique independence fighters who had come to lend a hand to the carers. They had all come to say no to the health pass and to compulsory vaccination from 24 October, i.e. in eight days. This Saturday morning, the demonstrators and police disappeared. …At the Fort-de-France University Hospital, most of the hospital staff still refuse to be vaccinated. According to the hospital’s management, officially 20% of the staff have been vaccinated. Its director warns his team. If there are fewer carers, the hospital will not be able to function normally. The situation is all the more critical because for several weeks now, other patients outside Covid and the emergency room have not been treated due to a lack of available beds.”
17/10/21:
Interesting comment
Translation:
“Remdesivir, Astra, Moderna, are discreetly “exfiltrated”, after having been approved by health authorities on the basis of a single study, that of the lab, of course without any bias or conflict of interest [sarcastic], while excluding products studied by independents, without any conflict of interest. What are their criteria and working methods for making so many mistakes? You won’t know, because while these decisions should be transparent and recorded as required by law, they aren’t, and when we point this out to ministers, they don’t respond.”
16/10/21:
On Antibody Dependent Enhancement (ADE)
Translation:
ADE in Israel, myth or reality?
Posted on 15 October 2021 by ZOLA
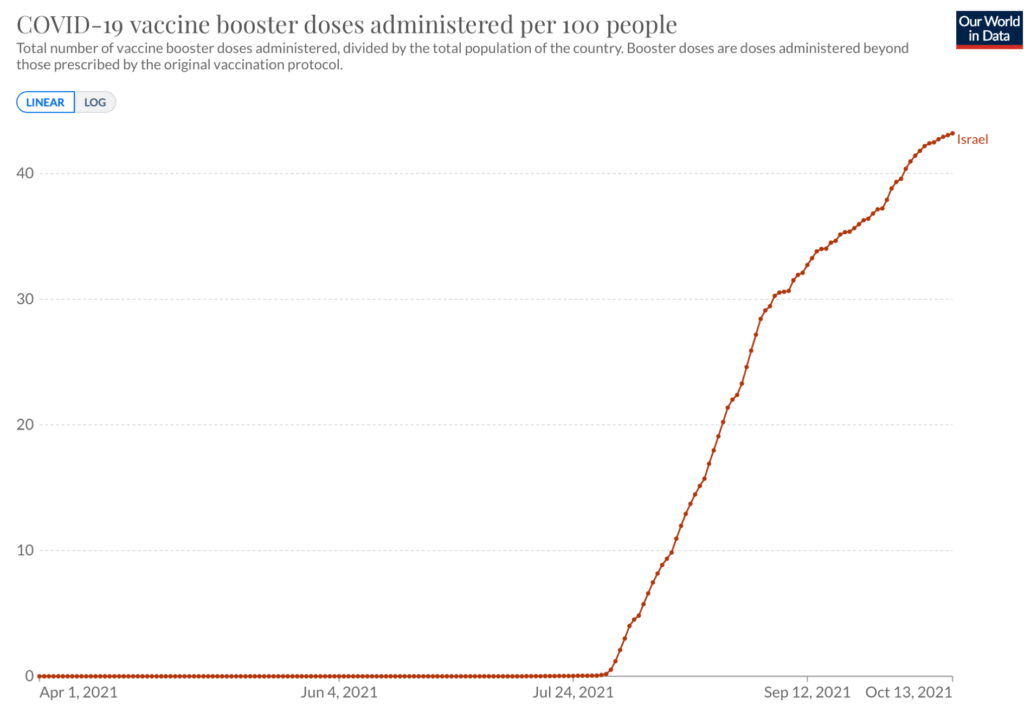
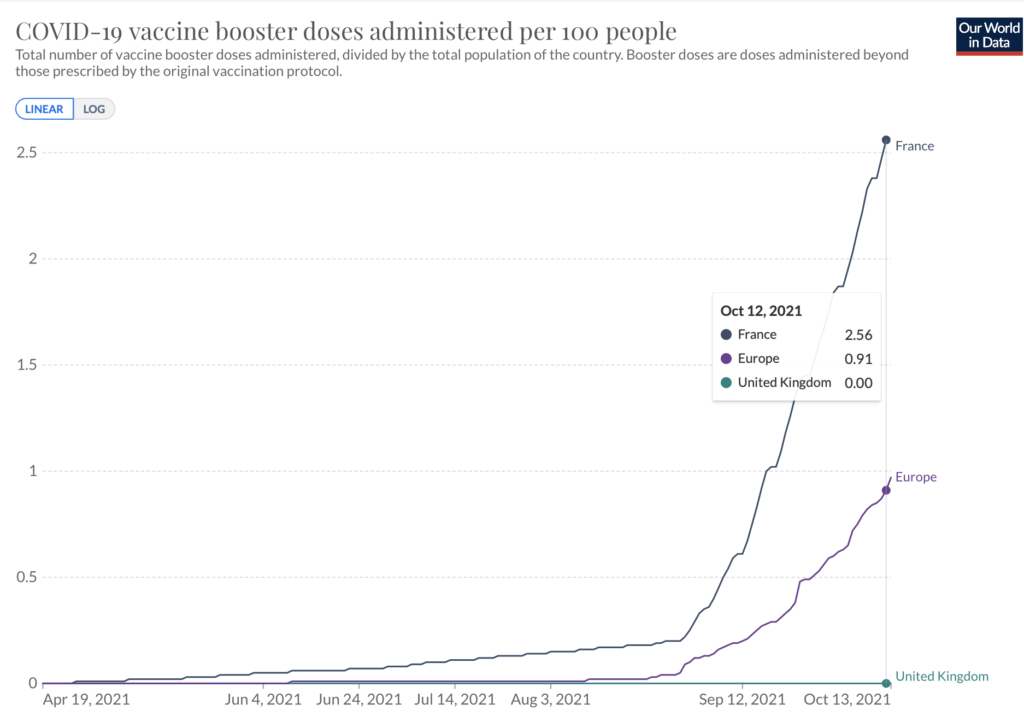
The WHO has always been cautious about the third dose of vaccine, advising against it several times in recent months. This did not prevent Israel from embarking on this adventure at the end of July, with other countries like France following suit. Our President had said that we should follow what was happening in Israel, a pioneer in mass vaccination, but unfortunately following does not necessarily mean drawing conclusions, when you follow with your eyes closed instead of opening them.
Why is the WHO cautious? Only once did it come up with a bogus pretext, “to give our doses to poor countries”, but the problem is elsewhere. Is it because of the possibility of the ADE phenomenon? In Israel, what is the result of this third dose?
When we defend ourselves against an infection, we make antibodies. We make several because there are several proteins in the intruders to eliminate, and we also make several types of antibodies, all means are good. There are basically three types of antibodies:
Antibodies that are made but have no effect, either because the target is useless to neutralize or because it’s a dud. These antibodies are called neutral antibodies. They do not serve any purpose.
Effective antibodies, those that block or destroy the intruder, those that we try to obtain by vaccinating, and that we call neutralizing antibodies.
But there are also unwanted antibodies, which will play a bad role by helping the intruder. These antibodies are called facilitating antibodies, and are responsible for the ADE phenomenon, which can facilitate the work of the pathogen. During a reinfection, this pathogen will then have an ally in place.
So we have to go on observation, and Israel lends itself well to this. The country has just faced a last wave, just as considerable as the one of last year at the same time (1 month difference), whereas last year there was neither treatment nor vaccine, and currently two thirds of the population are largely vaccinated with two doses. Vaccine ineffectiveness? In our country, it seems that it is the fault of the unvaccinated, “who represent 80% of the hospitalized”. Unfortunately, for this to be true, they would have to be 3 to 4 times more affected than last year to obtain these figures.
Here is the curve of cases, superimposable to the one of deaths, it starts at the end of July and accelerates, as if the vaccine did not do anything.
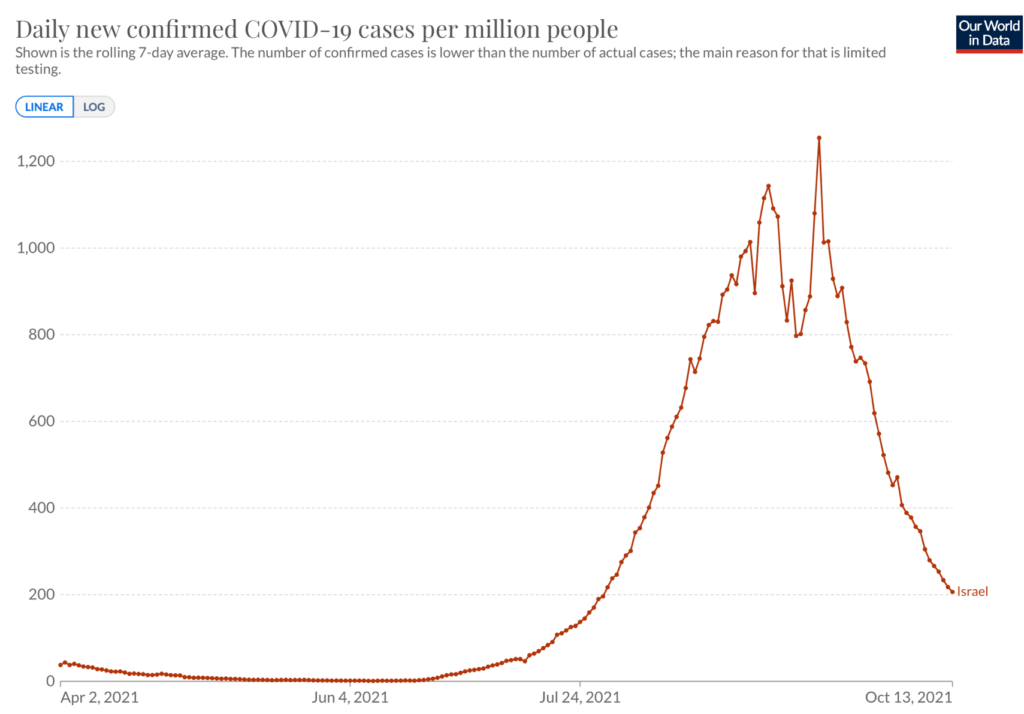
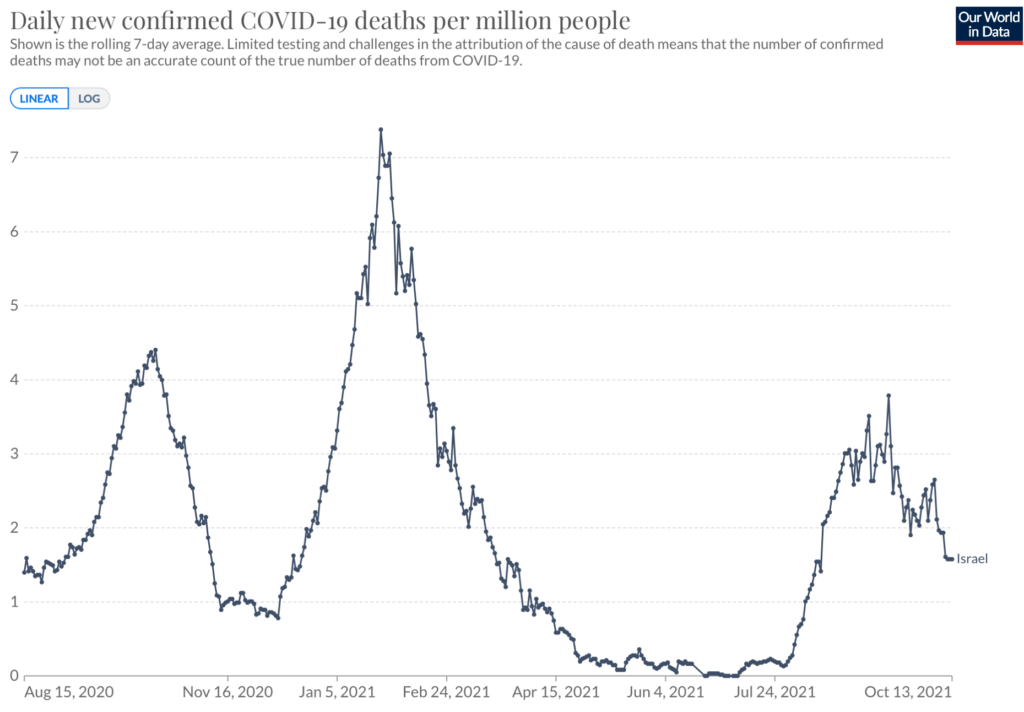
Israel justifies the third dose by the fact that vaccine immunity is exhausted over time, so it must be revived. But with an efficiency of 50%, what explains that we have as many deaths as without vaccines, if not the ADE? If this is not the case, I would like to be given a coherent explanation.
To finish, an extract, still from the Vidal :
Thus, most often, ADE occurs when the person has low circulating levels of neutralizing antibodies (insufficient or old vaccination, elderly people, not very symptomatic infection) or a low specificity of these antibodies, for example during cross immunity between two viral infections.”
15/10/21:
Podcast and transcript of conversation with Simon Elmer of Architects for Social Housing
How people who have been in the UK… everything that’s happened in this country… through various governments going back to say, the Iraq War, just to have a little cutoff point, but you can go way back further than that…Everything we’ve done in the Iraq War, the imprisonment of Julian Assange, the fiscal austerity, which is, you know, the financial crisis, the housing crisis, all this sort of stuff. We all know that it’s been done on a pack of lies. We know that our press has lied to us repeatedly, over and over again, and I’m not talking about little lies, I’m talking about really big lies. The lies that Iraq had weapons of mass destruction and stuff like that… Suddenly these people believe everything the media say. That’s something that I’m trying to understand. How that has happened.Because it’s that, it’s the collaboration… This is not a conspiracy, this is a collaboration at every level … I think that is something which is more important to understand than why Bill Gates wants to run the planet……
But it also shows kind of the point you were making, it shows that the middle classes implement – they administer – capitalism. They have been financially incentivized to comply with it.They’ve also got a class consciousness, I think. An allegiance. These people are… if they were not themselves, their parents were doctors, were teachers, they were lecturers, they were in the media or are in the media. These are their industries.You know, my partner, Geraldine Denning who is the co-founder of Ash – Architects for Social Housing – she also teaches architecture at Leicester University. And last year, the university was really putting pressure on her to become a kind of policeman. To make sure that students were wearing masks in class were observing social distancing, and also were signing up to a kind of pilot testing, a lateral flow antigen testing pilot, which had been introduced into Leicester University… And she said I’m not doing any of these things. And we wrote up together a letter that we sent around to every student in her department, but also every teacher, fellow lecturer in the university. I mean in the architectural school, of which there were about a hundred. She didn’t know all of them… but there are a hundred lecturers in the School of Architecture. And not a single word. Nobody responded at all.”
Superior Natural Immunity to SARS-CoV-2 (?)
Not yet listened to this podcast, and not sure how valid it is nor how far scientific/medical reasoning and facts can help the fight against the 21st century industrial medicine spectacle, as many people are becoming even more delusional and ideological as this continues (that is, even more than let’s say a year ago) – toward the scientific/medical facts and conditions as well as about the political-economic powers that delineate our relation to the scientific/medical facts and conditions). Anyway, this claims to show:
-
- How the official ignorance of natural immunity illustrates how public vaccine policy is not about public health but about power, control, and profits for the pharmaceutical industry.
-
- How it is demonstrable that public health officials are deliberately lying about what science tells us about natural immunity.
-
- How the vaccine propaganda began while the vaccines were still under development with false claims in fearmongering media headlines that natural immunity wanes rapidly.
-
- How scientists propagating the message that antibodies equal immunity and therefore loss of circulating antibodies equals loss of immunity knew that this was false.
-
- How, with measles, the inferiority of vaccine conferred immunity and the loss of natural “exogenous boosting” has resulted in mothers today being less well able to convert passive maternal immunity to their babies.
-
- Why natural immunity must be considered an opportunity cost of vaccination.
-
- What “original antigenic sin” is and why everyone should be aware of the potential for this phenomenon before deciding to get a COVID-19 vaccine.
-
- How mass vaccination could actually impede the development of herd immunity.
-
- How mass vaccination could put evolutionary pressure on SARS-COV-2 resulting in the emergence of an “escape variant” (not unlike how the pertussis vaccine has resulted in the emergence of strains lacking a key antigen component of the vaccine).
-
- Why getting an annual flu shot might actually increase the risk of influenza illness in the long run.
-
- How in 1976 public health authorities warned of an influenza pandemic and pushed a mass vaccination campaign, but no pandemic occurred, and the vaccine was shown to cause Guillain Barre Syndrome, a polio-like paralytic disease.
-
- How the 2009 pandemic influenza vaccine in Europe was found to cause narcolepsy, another autoimmune disease.
-
- How studies have found that pre-existing cross-protective T cell immunity against SARS-CoV-2 from prior infection with coronaviruses that cause the common cold.
-
- How the media cherry pick studies to propagate the most alarmist fearmongering headlines.
-
- How the public health establishment and media have propagated the claim that more antibodies equal better immunity, even though a high level of antibodies is actually associated with more severe COVID-19 (independently from age).
-
- How antibodies are neither sufficient not even necessary for immunity to SARS-CoV-2 (just as with measles).
-
- How the public health establishment has propagated the claim that vaccines offer better protection against variants based on studies that completely ignore the role of cellular immunity as well as immunologic memory.
-
- How the CDC lies by omission by persisting in saying that people who’ve recovered from infection still need to get vaccinated because scientists don’t know how long natural immunity lasts, withholding the fact that studies have shown that infection induces recognized markers of very long-lived immunologic memory.
-
- How some studies have shown that vaccination can have a detrimental effect for people with pre-existing natural immunity, through what is sometimes called “immune exhaustion”.
-
- How the scientific community knows that the CDC is deceiving the public, yet most scientists are either silent or complicit in the big lie, illustrating the thorough corruption of science from government involvement in “public health”.
-
- What “antibody dependent enhancement” is and why it remains a concern for COVID-19 vaccines.
-
- How, to support its policies, the CDC cites studies that either don’t support or directly contradict its claims.
Long Island father refused right to see his 3-year-old daughter unless he gets the jab
13/10/21:
“Beyond industrial medicine” – interesting text by Eisenstein
“…What lies outside the debate about vaccine safety? Effective natural and alternative treatments for Covid. Superiority of natural immunity to vaccine-induced immunity. The “terrain” of infection: why some people experience serious illness and death, and others do not. The positive role viruses, even pathogenic ones, play in health and evolution. The decline of virulence over time. The sociological implications of handing body sovereignty over to government authorities.
Basically, vaccines are a way to keep society-as-we-know it functioning as usual. The idea is, “Everybody get the jab and we can go back to normal.” It is much like psychiatric medications. Taking for granted a society that makes vast numbers of people miserable, maybe we need those drugs to keep them happy, or at least functioning. They can get back to normal—the life defined by society’s norms. Yet that life is what may have made them miserable to begin with. Similarly, what we have known as normal includes the conditions that result in needing (arguably, anyway) the jab in the first place.
Normal has been a society where autoimmunity, addiction, diabetes, obesity,6 and other chronic conditions are at epidemic levels. This epidemic is actually quite new. In the 1950s, the prevalence of diabetes in the United States was a tenth what it is today. Obesity was a third. Autoimmune diseases were medical rarities. As most Covid deaths are in people with diabetes and other chronic conditions, the whole context of vaccine policy includes conditions that are historically aberrant.
Normal has been the disempowerment of people to maintain their own health themselves and in community, making them dependent instead on experts to do things to them. The “patient” is passive, patiently enduring what the expert doctor does to her…Normal has been the marginalization of holistic and natural healing modalities that offer effective treatments for Covid and most other conditions. Oops, that sentence will get this flagged as misinformation. Where’s the data, Charles? Well that is part of the problem. Society has not devoted the vast resources into researching and developing herbal, nutritional, vibrational, and other unorthodox therapies that it has into pharmaceutical ones. They don’t fit the funding system and they don’t fit the paradigm. So, evidence at the level of multiple large-scale double-blinded placebo-controlled trials is scarce. Moreover, since many alternative therapies depend on unique relationships between therapist and patient, individualized treatments, or active work by the person being healed, they are inherently unsuitable for standardized trials. Standardized trials that produce the aforementioned “data” require the control of variables. They are part of what I’ve been calling industrial medicine—”industrial” is all about standardization, control, quantification, and scale..”
11/10/21:
Brief but basic anarchist response to the current situation
This French text was rejected by the anarchist journal “Le Monde Libertaire”.
Translation:
The sources of health and the (forgotten) anarchist legacy
Today we are witnessing the development of a project of control and submission of populations, whether rich or poor.
This project implies the dispossession of our autonomous capacities to take care of our lives and those of our loved ones. And all that the broad term health includes.
The states and the different forms of big capital have taken a gigantic step forward in this direction, thanks to the support of the media: the management of the Covid-19 epidemic is an example of how power can lead entire populations towards a new form of domination by acting on something as elementary and intimate as our health. With this in mind, and maintaining a libertarian stance, how can we address this delicate and crucial issue? We should not, as has been the case until now, limit ourselves to denouncing the capitalist expropriation of medicine or pointing out the way governments use health measures to put an end to our fundamental rights. All this is real, but it is not enough to define the absurd barbarity towards which our governments are leading us with great strides.
After more than a year of media confusion and state propaganda, we can now guess that the horizon that is emerging is that of a population that is periodically vaccinated or provided with health passports that allow them to circulate and lead a “normal” life. It goes without saying that in no case is the state’s aim to protect the health of its subjects, but rather to establish its hegemony a little more by dispossessing us a little more of our personal responsibility and to maintain the same harmful environmental conditions in which we live every day.
States, as we know, function as large machines to which we must adapt or die. In this sense, diseases and epidemics are seen only as external biological threats, unrelated to the lifestyle and hygiene to which people are subjected. The infectious agent is an obsession and the organism is a passive element that can do nothing but be assisted from outside by means of a supposedly effective scientific medicine.
However, it is this schematic and simplistic view of illness that was denounced by emblematic figures of anarchism at least a century ago. We are thinking, for example, of a book such as La ecología humana en el anarquismo ibérico by the historian Eduardo Masjuan, which shows the importance that an integral vision of society and nature had for anarchism in the period before the Spanish Civil War. Rather than artificial defence against the infectious agent, the important thing for naturalistic anarchism is to spontaneously develop the body’s defences through the practice of hygiene, physical activity and appropriate nutrition. Beyond this, naturalistic anarchism denounced how poor working conditions, housing, childbearing, etc., of the working classes were factors in the spread of contagious diseases such as tuberculosis and cholera. The improvement of these conditions through social struggles, rather than vaccination, was responsible for the reduction of these diseases in urban and industrial areas. Today, populations are subject to other types of environmental and hygienic factors, which environmentalists and researchers in nutrition and hygiene have been denouncing for decades, without meeting with much response. Despite one or two centuries of “scientific” and medical progress, the average health of the population is precarious. And we note that at least part of anarchism is not insensitive to these types of concerns. In particular, one can see how some anarchist currents, unlike many of today’s epidemiologists and media agents, have taken the issue of health seriously, attacking the problems at their roots, or at least attempting to do so.
Today, these simple lessons seem to have been forgotten. We expect mass vaccination to get us out of this hell, while mass vaccination programmes are part of this hell of hostile environmental conditions and harmful lifestyles that the state and capital impose on us. We also know that despite the media’s message, scientific controversy about the effectiveness of vaccination campaigns persists, not to mention the possible harmful side effects. The obsession with the external infectious agent is gaining ground against the richer and more ethical concept of health.
Naturist anarchists such as Dr. Isaac Puente (1896-1936) [see note], insisted that the important thing to take care of health was not to consider the masses but rather people: the autonomous appropriation of each person’s health. An essential responsibility that is nowadays brutally threatened. The sources of our health are not, and cannot be, in the opportunistic dispositions of governments or in the programmes of big pharmaceutical business.
The forgotten heritage of anarchism offers us a key: let’s take care of our health on a daily basis, and at the same time let’s fight to abolish the unhealthy conditions in which we are kept, let’s not wait for the medicine of the State and of capital to impose a new type of misery on us.
José Ardillo
Note: Isaac Puente was a vital figure of Spanish anarchism in the 1930s. He was the author of the famous El comunismo libertario, the theoretical basis that was approved in the congress in Zaragoza in May 1936. He was assassinated by the fascists at the beginning of the war.
How Thailand is using a ‘cheap and effective’ traditional herbal medicine to treat coronavirus
Not at all sure how effective this is as it’s only being used for the asymptomatic or mildly infected.
10/10/21:
Israeli Ministry of Health actively suppressing complaints on vaccine side effects
Translation:
“The Ministry of Health is in a panic. These “anti-vaxxers”, who talk all day about their side effects, are sabotaging the booster campaign. The hate-mongering and dividing “Stealing My Acme” campaign creates a boomerang effect, and only makes it that even those who have considered getting vaccinated for a third dose realize that something bad is happening here, and it is not the virus. Actors, athletes and even journalists are already beginning to confess on Twitter and Facebook that they have contracted facial paralysis and autoimmune diseases, or that relatives to whom they preached to get vaccinated have contracted myocarditis after the previous doses, and are wondering whether to succumb to the third dose.
The hysteria in the ministry – which until two weeks ago was as complacent as a turtle in the meadow, especially after the High Court gave it the green light for the black pass – began on Black Friday (for them) when the FDA decided, after seeing the colossal data presented by the head of health services – who is responsible for implementing the booster policy now and by pure coincidence happens to lead Pfizer’s study in Israel, and also just happened to sign the state’s contract with Pfizer – an unequivocal decision that the entire population should not be boostered with a third dose until the age of 65. Their line of reasoning has shattered. Even the FDA already understands that the experiment simply failed, and that it is impossible to continue to boost the population forever.
What do you do, what do you do? Out of hysteria, the lights in the office were on all night. Within an hour they informed the media, who were momentarily confused and thought they were an investigative press and wrote that there was drama in the FDA, that there wasn’t any drama whatsoever – every message can also be seen upside down: you didn’t understand. It’s not that the FDA didn’t agree to authorize the booster for the majority of the population up to the age of 65. On the contrary, it is that the FDA *agreed* to authorize it for those aged 65 and over. The mouthpieces aligned themselves and went into action immediately, pumping up for days this amusing framing.
But bummer. The FDA’s message was internalized loud and clear. Even among a large portion of those who were already on the verge of succumbing to the booster threats.
So what do we do now? The FDA has sent the Ministry of Health to do homework: keep checking the effectiveness of the booster – on lab rats – us! And the lab rats rebel! Most of them may not say it out loud, but they just don’t come. So a genius mind there came up with a brilliant idea! Why not speak, nail the message to them? Vaccines are effective and safe. Roger. Out. That’s all you need to know.
It’s just that this is a reaction the brain-genius did not expect (why didn’t he expect? After all, the exact same thing happened to the Prime Minister of New Zealand): thousands upon thousands of reports on side effects, from heart attacks and paralysis to death [this is on the Facebook page of the Ministry of Health, as comments to their “the vaccines are effective and safe” post – Translator’s note]
Want to talk about side effects?
Come on, let’s really talk about side effects – and let’s start with the fact that Israel *does not* have a side effect monitoring system like in other Western countries – one that allows every citizen to view, read and understand the side effects that other citizens have reported, one that allows independent researchers to examine the data and see whether certain symptoms recur after the vaccine – a relationship that must be
tested to see if it is indeed causal.
There is no reporting system in Israel. What exists is a reporting *form* – not a reporting system, and this form is also lacking, and until recently there wasn’t even a place in it to fill-in the details of the reporter, not even his/her name – which testifies more than anything else to the fact that the ministry have no intention of examining the reported side effects and have not had one from the beginning.
Let’s talk about the Magen Avot [the reporting system for retirement homes – Translator’s note] and Maternity Reporting System, which was *shut down* in December 2020 – just at the time when the vaccination campaign in the elderly and in nursing homes began.
Let’s talk about the reporting system and the culture of reporting that you have instilled in the medical staff, when in most cases when a person comes to the hospital – with chest pain, with heart attack, with blood clots, with bleeding, with abortion, with stillbirth – no one even asks him/her if he received a vaccine in recent days.
Really, let’s talk about the side effects. Don’t TL;DR us anything [Too long; didn’t read (abbreviated TL;DR and tl;dr) is a shorthand notation added by an editor indicating that a passage appears too long to invest the time to digest it – Translator’s note]. Listen to the public. Let *you* get to know the data!
Or not. Just delete them in your usual wretchedness, and continue to believe that the bodies already piled up in the thousands can continue to be hidden in a pile.
It will not help you. Because the public has woken up, and the thousands of comments you have deleted have already been captured and documented. Do not silence the injured anymore.”
See also this.
“The real question that we have not yet answered is the safety data of an mRNA in young people vis-a-vis myocarditis,” Dr. Anthony Fauci, President Joe Biden’s chief medical adviser and the top U.S. infectious disease expert, said in a telephone interview. “The Israelis will relatively soon have that data because they’re vaccinating everybody in the country I think from 12 years old up, including their military recruits,” Fauci added.
8/10/21:
American and Chinese scientists planned to collaborate on creation of new coronavirus not found in nature
“The grant proposal, obtained by the analysis group DRASTIC last month, was submitted to the U.S. Defense Advanced Research Projects Agency (DARPA) in 2018 …While the grant was never approved, it provides further evidence that American and Chinese scientists were exploring gain-of-function research, in which scientists manipulate existing viruses to make them more transmissible and/or dangerous.”
For more on gain-of-function research, see part 4 of this.
7/10/21:
France, Guadeloupe (overseas territory): sabotage of hospitals in response to compulsory vaccination of health personnel
“The health authorities have denounced malicious acts in health establishments against the backdrop of the debate on compulsory vaccination of health personnel…Oil in the offices, glue in the locks and “malicious acts”: the health authorities of the department of Guadeloupe have denounced, Wednesday 6 October, “actions of sabotage” within health institutions, in the midst of virulent debates on the vaccine obligation. Some people “are carrying out sabotage actions inside the establishments”, said the director general of the Guadeloupe regional health agency (ARS), Valérie Denux, during the weekly update on the health situation. “They have been pouring drain oil into the human resources departments of the university hospital [of Pointe-à-Pitre] over the past few days; they are putting glue in the locks; they are blocking certain accesses,” she said, estimating that these actions lead to “disorganisation and even loss of opportunities for patients”. I understand that people can express themselves,” added Ms Denux, “but these are really reprehensible acts [that] can put you in danger. The debate on the health pass and mandatory vaccination is virulent in the archipelago, with social protest being expressed even in health establishments, notably at the Pointe-à-Pitre university hospital, where the majority of staff remain unvaccinated.”
5/10/21:
Slovenia, Ljubliana: further clashes with state over mandatory vaccinations
See entry for 30/9/21 for further info.
Talk about live and non-live polio vaccines in Africa
This says that live vaccines (in this case against polio) have an effect of boosting the natural immunity of the body. “Arguments have become black and white. Vaccines are good, vaccines are bad.There is no room for new perspectives. There is no room for our research findings …Non-live vaccines…have negative non-specific effects.They simply do not improve overall health as much as expectedbased on the protective effects,and, in fact, most of them have negative effects on overall health.…we’ve been accumulating data for 25 years nowshowing that vaccines have important non-specific effects.Yet, the world only focuses on the protective effects.Our research results are not quite yet accepted.And I’ve spent literally years, I think, pulling out my hairand speculating why it’s so difficultto get these promising results acknowledged.And I think the main reason is the polarised vaccine debate.The people who have the power to do something,to follow up and respond to these findings –the World Health Organisation and the health authorities,are all vaccine supporters.And in my interpretation,they are reluctant to accept our findingsbecause they imply the possibility that some vaccines may sometimes be harmful.So it is easier just to dismiss the whole thing.The vaccine skeptics, on the other side,may find that our observations on non-live vaccines confirm their worst fears –vaccines can be harmful –but they may be more reluctant to accept the beneficial effects.And their focus on the negative effectsmay make the vaccine supporters take an even more rigid stance.In my opinion, neither side is right or wrong.Both sides miss the new perspective.And meanwhile,the clock is ticking.Worst of all,we are missing out on the potential to save millions of childrenwith minor changes to the vaccination programme.And things are moving in the wrong direction.Live vaccines are being stopped;more non-live vaccines are being developed.For instance, live polio vaccine has already been replaced completelyby non-live polio vaccine in high-income countries. … the plan is to stop live polio vaccine completely by 2022and replace it entirely with non-live polio vaccine.Based on all the available data,this global switch from live to non-live polio vaccinewill be a public health disaster.“
3/10/21:
Obituary and reminiscence of Mexican anarchist who died of Covid
Not really directly relevant to this page, but put here because it’s a nicely written piece.
Sweden: Interview with Dr. Sebastian Rushworth in Sweden about lockdown and the virus (20 mins)
(see also this interesting response to some of this in the comments box below)
Just to note some of his points:
Apparently, before people started to be vaccinated, surveys of a random sample of the population, including obviously those who had not necessarily taken a PCR test (and therefore have avoided the official statistics of those infected by Covid), but who have Covid antibodies, “The general consensus now it that somewhere between 99.7% and 99.8% of people who get Covid survive it”. For the elderly and those with comorbidities it’s possibly 10%.
On “Long Covid”: if you get sick and spend a long time in an ICU, regardless of the reason (a stroke, heart attack, ME, etc.) there’s a significant possibility you’ll have long term symptoms regardless of whether you’ve had Covid or not. “Studies of those with sympotmatic Covid – after 3 months 98% are fully recovered”.
Sweden compared with Norway, Finland and Denmark: “If you look at any previous pandemic in the 20th century Sweden had a much higher death rate…So clearly there’s an underlying difference between Sweden and its neighbours…Some of the countries with the harshest lockdown measures also have the highest Covid fatality rates. Other countries that have taken a very mild approach can have a very low fatality rate. Sweden has a more urbanised population than its nordi neighbours. The nordi country that has the second highest rate of Covid is Denmark which also has the 2nd most urbanised population. So people are living more tightly together. Sweden has more interenational travel. We got a lot more Covid early into the pandmeic when the treatments were still being figured out…Finland, Norway and Denmark – they competely avoided the first wave – just because there’s less international travel. They didn’t get the virus into the country until the autumn of 2020 and by that timne we figured out better how to deal with Covid…Sweden also had an unusually low mortality rate in 2019 while its neighbours had a normal or higher mortality rate…Going into the pandemic Sweden had an unusually high number of frail people who would normally have died the year before but didn’t. Our neighbours didn’t have that. In a normal year Sweden has 0.9% of the population who dies. In 2020 that number was 0.95%…a pandemic which only increases mortality rate by 5% is not a very deadly pandemic…In all of Sweden at the moment there are roughly 200 people being treated in hospitals for Covid. This, in a country with 10 million people …I’ve seen more people who’ve been harmed by the the vaccine than by the virus in the last couple of weeks.”
Haven’t yet checked this information, but, judging by other things he’s said, it’s unlikely that he’s manipulated the facts. True, given the enormity of confusion and misinformation from so many people around this illness, I should maybe be more thorough in double-checking the various bits of research – and that goes for other bits of information related to Covid on this site, but that requires an enormous amount of patience and energy, both of which I lack at the moment.
Re. the first paragraph – “The general consensus now it that somewhere between 99.7% and 99.8% of people who get Covid survive it” – this clearly shows that Covid has been far more widespread than originally thought, and yet less dangerous than originally thought. It’s very possible that annual cases of flu are similarly underestimated since very often people don’t even report that they’ve got flu, particularly if it’s short-lived and with only a small fever.
France: anti-Health Pass demos throughout country…Pau: station and railtracks invaded
2/10/21:
Cause of death after COVID-19 vaccination & undeclared components of the COVID-19 vaccines
Not sure how valid this long (2 hours 38 mins) banned-by-Youtube video, presenting the findings of various autopsies and other stuff, is as I haven’t researched yet the people involved nor have I seen more than a small bit of it.
1/10/21:
Vietnam, Ho Chi Minh City: clashes with cops following end of Covid-restrictions
Australia: whilstle-blowing nurses speak about their experiences of vaccinated patients
Detailed French article about Israel indicating some curious statistics
“We will start by seeing that there is absolutely no detectable overall mortality problem in Israel since 2020, i.e. since the West started to publicise people dying or becoming ill from respiratory infections and whose cause is attributed to Covid-19. Mortality has always increased in Israel during the winter period and in 2020 remained at levels comparable to previous years. Thus, all measures taken could never be motivated by a measurable impact on mortality. No more Israelis are dying than before. There has never been a massacre.
We will see what happens to mortality during the vaccination period. We will see that in Israel, as for all the countries for which we have data (as we have shown in the video or the article summarising all the European data), mortality increases during the periods when mass injections are carried out. For older people, there is some doubt as to whether there is a correlation or a causation, because the injections take place in the winter period when mortality is also usually high. On the other hand, it is very unusual to observe an increase in mortality among young people. We will see that this higher than usual mortality corresponds to about 3.8 deaths per 100,000 complete injections over the period for 20-29 year olds, 2.3 for 30-39 year olds and 1.4 for 40-49 year olds, whereas for these age groups, mortality during the Covid-19 period is undetectable. This work was taken up again following the analysis carried out by Dr. A. Henrion-Caude and Dr. S. Ohana and found the same results.
Finally, we will see if there is a link between the injections and the number of positive cases reported by the laboratory tests. First, we will see that the number of tests varies enormously. It is therefore quite normal to have more positive cases when the number of tests is increased. Similarly, the type of tests changed this summer with the screening strategy. In France, as elsewhere, this change in measurement with more variants considered positive necessarily leads to an increase in positivity without it meaning that a disease is spreading. Finally, the implementation of the Green Pass in Israel implies, as in France, that people who have not received an injection do far more tests than those who have received two injections. Therefore, we expect to have a much higher proportion of positive cases among those who do not have a Green Pass. We will see that if we take these biases into account, the Israeli data do not show a significant difference between those considered vaccinated and those who did not receive an injection. For Israel, the proportion of people considered vaccinated and positive for Covid-19 is the same as the proportion of people considered vaccinated in the general population.
…over 30 days Israel recorded 5,304 deaths in January 2021. Taking the January 2017 population to the January 2021 population, there would have been 5,374 deaths [per month]“
Leave a Reply