Covid: Ivermectin superior to vaccine
Translated from here
SF note: I’ve put this here to counter the whole absurdly disgusting vaccination programme; it should be obvious that I don’t agree with the ideological aspects of this text – its support for pre-Covid normality in the form of normal levels of wage labour, for instance.

Posted on March 25, 2021 by Gérard Maudrux
By agreeing to take into consideration the results of 8 meta-analyses around the world and the numerous testimonials from treatment providers, by comparing all the practical, medical and economic aspects of a massive vaccination campaign or treatment with Ivermectin, the benefit of Ivermectin would be considerable.
THERAPEUTIC
The situation: today we are in a pandemic phase, with a number of patients, some of whom will develop a serious form, leading to saturating hospital services, resuscitation, with a number of deaths, not to mention the collateral medical damage with all those presenting other pathologies that cannot be treated. Anticoagulants, corticosteroids, Remdesivir, Bambalaba and others are totally insufficient to stop this infernal machine, which we are trying to reduce by successive confinements, with considerable economic and social consequences.
The treatment: administer the vaccine from the first symptoms, as soon as you are hospitalized, in intensive care, will give you no results. Give Ivermectin, you improve the situation with recovery time twice as quick, and hospitalizations and deaths divided by 4 to 5. These results are found in all the meta-analyses worldwide: Kory (USA), Hill (GB), Nardelli (Italy), Guillausseau (France), Bryant/Lawrie (GB), Cobos-Campos (Spain), C19Ivermectine, Ivmeta, etc.
All, without exception, say the same thing. What do those who refuse to read this oppose? Nothing, they just don’t talk about it. Look this week once again at the publications of Inserm, the European Agency, Costagliola: they have been blocked for 1 year on a Petri dish, refusing to discuss its effect on human beings. Professor Changeux, an eminent French specialist of world renown and nobel prizewinner for his work on acetylcholine, nevertheless informed them, directly and on several occasions over the year, that the innoculated doses used in humans are totally effective in eradicating Sars. -Cov-2 as much as they are for animals.
Advantage Ivermectin.
PROPHYLAXIS
Vaccination is a prophylactic treatment, it is not meant to treat illnesses (with rare exceptions such as rabies, due to the long incubation of the disease, longer than the immunity that can be acquired by the vaccine). It is given to prevent people getting sick. Its efficiency ? From 60 to 90% depending on the vaccine. The 90% efficiency is starting to be considered doubtful (Doshi, Ben Cheikh) as Pfizer did not provide the raw data – the FDA also criticizes AstraZ, for its data. Let’s admit to an 85 to 90% efficiency so as not to get stuck in this controversy (I am also aware that it is accepted by everyone that vaccines are less effective in the elderly, the main targets, so 80% would be more correct).
For Ivermectin prophylaxis, 12 studies on the subject show 85 to 100% (Carvallo) efficacy. 92% for the latest French meta-analysis by Guillausseau, who was formerly a member of the AMM committees, and therefore knows how to analyze these data.
Conclusion: equality with regard to prophylaxis, with however an advantage for the vaccine, the administration of which would protect people for 6 months (to be discussed), against 4 weeks for Ivermectin. This difference will be erased, however, once the long-acting form of Ivermectin is developed by Medincell, which is currently under development.
RISK
Vigibase is the WHO database which, for 30 years, has been collecting the adverse effects of all drugs, communicated by the various pharmacovigilance agencies of more than 130 countries adhering to WHO.
We note: Ivermectin, in 30 years, 4,704 adverse effects, 16 deaths, for 4 billion prescriptions. Comirnaty (Pfizer), in 4 months, 333,818 adverse effects, 2,435 deaths, for 3-400 million prescriptions.
Ivermectin is one of the safest drugs in the world (in comparison with paracetomol, which has had 161,068 side effects, 3,690 deaths in 30 years). It has been tested at 10 times the dose, with no problem. You can imagine that many of the disputed post-vaccine accidents are not all in this database
Advantage Ivermectin.
PANDEMIC CONTROL
France and Europe (and others) are counting everything on the vaccine, unsupported with early treatment, to stem the pandemic. We realize that the process takes a long time to put in place, and in addition to all the accidents that are increasing, if it takes 6 months to try to obtain sufficient collective immunity, we may, I’m afraid, have to re-vaccinate if the former lose their temporary immunity. We can see that in our country with 10% of people being vaccinated does not reduce the epidemic by 10%, which continues to grow, and that must be supplemented by confinement/lockdown in the absence of appropriate medical treatment.
However, control can be obtained more quickly with Ivermectin, without having to carry out a massive campaign as with the vaccine, and without having to treat people every 4 weeks if we want to do prophylaxis. Indeed, it suffices to treat symptomatic cases to relieve the hospitals, and to systematically treat not the entire population as for the vaccine, but only all contact cases, which, given the efficacy in prophylaxis, would prevent them from developing and dissipating transmission of the disease, so it would stop the epidemic. This cannot be done with the vaccine, which does not protect contact cases before they develop the disease, and does not prevent them from passing it on to others.
In Brazil, an agro-food company concerned with meat brought the situation under control with 12 000 employees in 1 month. Remember the frightening outbreaks in slaughterhouses.
Advantage Ivermectin
LOGISTICS
We have seen the time it takes to produce and distribute the vaccines. Logistics, given the problems associated with keeping the vaccine at a constant refrigerated temperature, are heavy, slow and expensive. None of that with Ivermectine. The production lines are there (human but also with veterinarians – it is the same molecule), and for distribution, it is no more complicated than for paracetomol.
Advantage Ivermectin.
ECONOMIC
The refusal to consider early treatment of Covid leads to the third confinement/lockdown. With its economic consequences running into the hundreds of billions, tens of thousands of small and medium-sized businesses that will not recover, years of worsening unemployment, etc., the list goes on and on. Conversely, a campaign with Ivermectin, from the contact cases onwards [SF note: ie in relation to those who would normally have had to stop work because of having been in contact with someone who’s been diagnosed with Covid], does not require stopping people from working, and the serious forms becoming few and far between, giving no problems for hospitals and no need for confinement.
Advantage Ivermectin.
SOCIAL LIFE
I will not dwell on the consequences on social life, disrupted human relationships. We have not finished looking at the consequences, with depression, suicides, unemployment and its effects, increasingly severe aggressivity inside and outside homes, schooling, etc. All of this is not related to Covid, but to confinement/lockdown, and is therefore not avoided with the vaccine, but could be avoided with Ivermectin.
All this, of course, supposes that we listen to, that we watch, that we read about the work done in many countries, by several hundred doctors, on tens of thousands of patients, analyzed and published by hundreds of analysts from different specialties. You still have to have the intellectual capacity to do this, which seems to be lacking for many people who think they are smarter than others. Better to have an image of intelligence than genuine intelligence, as Montaigne wrote.
SF note: The drug regulator in France – INSERM – has refused Ivermectin as a preventative medicine for Covid saying that there haven’t been enough trials. Catch 22: it has prevented such trials from being pursued.
Added 3/5/21:
DeeplTranslate of “Ivermictine – victim of sophistry”
Posted on 5 April 2021 by Gérard Maudrux
If paralogism is an unintentional error in reasoning with no intention to mislead, sophistry is a deliberately false reasoning, which, despite an appearance of truth, is deliberately designed to deceive or delude.
Sophists, the originators of the word, were thinkers who developed a rhetoric whose main purpose was to manipulate an audience. They were denounced by Aristotle, Socrates, Plato and other philosophers.
 “Sophistry is defective reasoning despite the appearance of logic”
“Sophistry is defective reasoning despite the appearance of logic”
“In other words, it’s a mental trap and rather dishonorable way of convincing”
sophistry course: https://slideplayer.fr/slide/6251896/
or https://slideplayer.fr/slide/1135896/
The conclusions of the EMA, the WHO, the ANSM concerning Ivermectin, (and who know perfectly well its strong presumption of efficacy), as well as the articles that follow, are presented as rigorous and logical demonstrations, but they are only sophisms made up of a true or allegedly true premise, arranged in a seductive but deliberately erroneous reasoning, which does not respect the rules of logic. Fallacies are difficult to refute if one does not master the facts and logic.
Wikipedia describes about forty different fallacies. All our authorities already practice the argument of authority, argumentum ad verecundiam: Ivermectin is ineffective because I have decided so, and what is not necessarily a truth at the beginning, then becomes for all the press a “generally accepted truth”, moreover no need to look for or demonstrate, “since it is the WHO that says it”. This is how everyone said at the beginning that masks were useless, it was a truth because the WHO said so.
The most used fallacies are those of generalisation. When there are several dozen favourable studies and you want to show the opposite, you take only one, you take out only a part that could lead you to believe that it is ineffective, and you say that it does not work by generalising. You don’t need to look at other studies, it doesn’t work. We have seen this technique in many articles and decisions. For example, ongoing studies on Hydroxychloroquine were stopped on the basis of a single study, which was known to be flawed, and all the others were swept aside. Dame Costagliola of Inserm thus denies the efficacy of Ivermectin, generally citing only one study, which moreover has nothing to do with it, and she generalises.
There is a manipulative fallacy systematically used by agencies to ignore results: the use of a “reservation of use” as truth, when it is only a reservation of use, not a fact or a demonstration. Thus, in the current atmosphere of permanent suspicion and criticism, studies and reports end, whatever the result, with : “we see this, but perhaps it needs more study to confirm it”. So Andrew Hill says that it works at 80%, which is no mean feat, and ends with the classic “formula”. The sophist will only remember this formula: “insufficient study, more studies are needed to decide”, allowing him to ignore the very result of the study. As Tess Lawrie said in an interview: “You can argue about the bias of this or that study, you can argue about the level of efficacy between 75 and 85%, but what is not arguable is the efficacy itself”.
The logic of sophists
Thus, the ANSM uses this reservation of use to assert that Ivermectin has no action in prophylaxis. It cites only one study out of a dozen, that of Berehal (41 cases!!!). I quote the conclusion of the study available here: “Two-dose prophylaxis with ivermectin of 300 μg / kg with an interval of 72 hours, was associated with a 73% reduction in SARS-CoV-2 infection in HCWs for the following month. Chemoprophylaxis is relevant to contain the pandemic”, and the conclusions of the ANSM: “the authors concluded that taking … was associated with a reduction in infection ….. However, they stressed the need for confirmation by longitudinal or interventional studies.”
The only thing that counts is the reserve of use, and the ANSM adds the argumentum a silentio, diversion of attention or omission (“vicious indifference” according to Mill): exit the Carvallo study on 1,200 carers with 100% effectiveness, exit the experiment on 12,000 employees at GTFoods with total eradication of the epidemic in a high-risk and permanently affected company. Then the press will pick up on this: “it’s ineffective in prophylaxis, the ANSM says so”. Argumentum ad verecundiam, quoted above, which uses the reputation of a source to validate the conclusion. Pure manipulation of a study, to demonstrate the opposite of what the study states, then taken up by the press.
However, the texts provide for the use of the drug in the case of “presumed efficacy”, without mentioning any proof or level of efficacy, which the ANSM misuses by taking into account only the reserve of use. Moreover, the sophists are unscrupulous, it’s part of their rhetoric: they gave a RTU to Baclofen for alcohol addiction without any scientific study, and other recent RTU and ATU on the strength of 2 studies without proof of effectiveness and without taking into account the reserve of use. I will detail in another post all the studies put forward by the ANSM, such as that of Médina, which is considered by many to be of the level of Mehra and Lancet, given the errors, which seem to have escaped the authors. At this level, using this is no longer sophistry, but incompetence (or taking the readers for fools).
There is also the sophism very dear to the Castafiore of Inserm, with the in vitro study that “demonstrates” that it does not work in vivo. She uses a version of the argumentum a silentio: there is a bias in the in vitro study, which allows her to assert that it doesn’t work in humans, which is completely unrelated. Yet every serious scientist knows that the absence of proof is not proof of absence. Inserm should know this too, but prefers to play it up.
Another execrable sophism widely used by the press is the reductio ad Hitlerum which Hydroxychloroquine suffered from last year: Trump and Bolsorano defended HCQ, which is true; Trump and Bolsorano are disreputable, which is true; therefore HCQ is disreputable, which is a false deduction. We’ve just done it again with Ivermectin for the last 8 days in the mainstream press: Le Pen, Dupont Aignan, Asselineau,.., defend Ivermectin, so Ivermectin is far right.
Let’s not forget the sophisms that consist in denigrating opponents by attacking people (argumentum ad personam) rather than the facts they expose (ad hominem). Thus, doctors who treat in the first instance are made to look like bad doctors who do anything, who can be dangerous and are therefore prosecuted by their Order or summoned by their ARS. Those who oppose the official doxa are nothing but conspiracy theorists and charlatans taking advantage of the distress of citizens.
To conclude, the argument that kills, argumentum ad ignorantiam: “if there was a treatment that worked, we would know about it”, an argument dear to the bewitching Karine Lacombe. We hide the truth, then we affirm that it doesn’t exist, since we can’t see it!
Yes, sophistry can kill
Aristotle, Socrates, Plato, where are you? You unmasked the sophists in your time. They are back, in force, they are everywhere, most of them trained in a school where the great oral consecration is a monument to the glory of sophistry. We have no one in our elite to defend truth and common sense as you did. Come back soon.
https://blog-gerard.maudrux.fr/2021/04/05/livermectine-victime-du-sophisme/
PS:
Added 8/7/21 – mentions of ivermectin on this site, put all in one place for convenience:
Ivermectin
Ivermectin: Can a Drug Be “Right-Wing”?
I’ve reproduced this article because you can only access the whole of it if you pay for it. It’s about how hospitals in the US fought hard, hiring expensive law firms, at times going to extraordinary lengths to refuse treatment using ivermectin even with dying patients who’d exhausted all other options, and even though ivermectin had been shown to be very helpful in aiding recovery in the patients who were then subsequently refused it. Also about how this potential Covid-19 treatment has become hostage to a larger global fight between populists and anti-populists.
“At Edward-Elmhurst hospital in Chicago, a 68 year-old named Nurije Fype was admitted, put on a ventilator, and again, as all other treatments failed, her family got a judge to order the use of ivermectin. Lorigo claims the hospital initially refused to obey the court order, which led to the filing of a contempt motion, which in turn led to a pair of counter-motions and another confrontation before another befuddled Judge named James Orel. “Why wouldn’t this be tried if she’s not improving?” the Chicago Tribune quoted Orel as saying. “Why does the hospital object to providing this medication?” “He basically said, ‘What do you have left?’” Lorigo recounts. “No one would administer the ivermectin. It’s as safe as aspirin, for Christ’s sake. It’s been given out 3.7 billion times. I couldn’t understand it.””
Why Has “Ivermectin” Become a Dirty Word?
“On December 8, 2020…the Senate’s Homeland Security and Governmental Affairs Committee held a hearing on the “Medical Response to Covid-19.” One of the witnesses, a pulmonologist named Dr. Pierre Kory, insisted he had great news. “We have a solution to this crisis,” he said unequivocally. …Kory was referring to an FDA-approved medicine called ivermectin. A genuine wonder drug in other realms, ivermectin has all but eliminated parasitic diseases like river blindness and elephantiasis, helping discoverer Satoshi Ōmura win the Nobel Prize in 2015. As far as its uses in the pandemic went, however, research was still scant. Could it really be a magic Covid-19 bullet? Kory had been trying to make such a case, but complained to the Senate that public efforts had been stifled, because “every time we mention ivermectin, we get put in Facebook jail.” A Catch-22 seemed to be ensnaring science. With the world desperate for news about an unprecedented disaster, Silicon Valley had essentially decided to disallow discussion of a potential solution — disallow calls for more research and more study — because not enough research and study had been done. Once, people weren’t allowed to take drugs before they got FDA approval. Now, they can’t talk about them.…”
https://blog-gerard.maudrux.fr/2021/06/10/les-miracles-de-livermectine/
“Another miracle is the day after day confirmation of what happened in India, in the states which used Ivermectin, with very rapid resolution of a wave announced by all the media as a disaster that was going to wreak havoc, the media which has since been silent on what is happening. Total blackout. Uttar Pradesh has fallen to less than 1000 cases / day, population 3 times the size of France, which would make 300 cases here, at a time when we are happy to go below 5,000 cases / day! Ditto in states like Delhi and Goa. These 3 states have reduced the cases by 98% compared to the peak at the end of April (37,000 cases for Uttar Pradesh, 28,000 for Delhi).
Since then there has been war in this country between the various national medical authorities under pressure from the WHO and Merck, with press releases authorizing or banning ivermectin. They have gone mad to see these results, but the responsible states do not budge and maintain their position. The Ministry of Health, after authorizing in a protocol, wants to now ban all early treatment. It should be noted in passing that the Minister of Health has been President of the WHO Executive Boardsince May 2020, and that the WHO immediately issued statements to advise against Ivermectin from the start of treatment, a complaint has also been made. filed on this subject, non-assistance to a person in danger is characterized. We then received a statement from the WHO congratulating itself on having intervened in this state to reduce the epidemic, by supervising 2,000 teams and distributing treatment kits, being careful not to say what was in them. Ivermectin, of course, but this product does not exist for the WHO. And more recently, we were treated to another victory press releaseafter the supposed ban (not yet very clear). The WHO, which congratulates itself when we do not give treatment, welcomes the ban on the treatments it has distributed. Incredible !
Finally, a quick comparison between a country that uses ivermectin, and a country that refuses it so as not to interfere with its vaccination campaign.
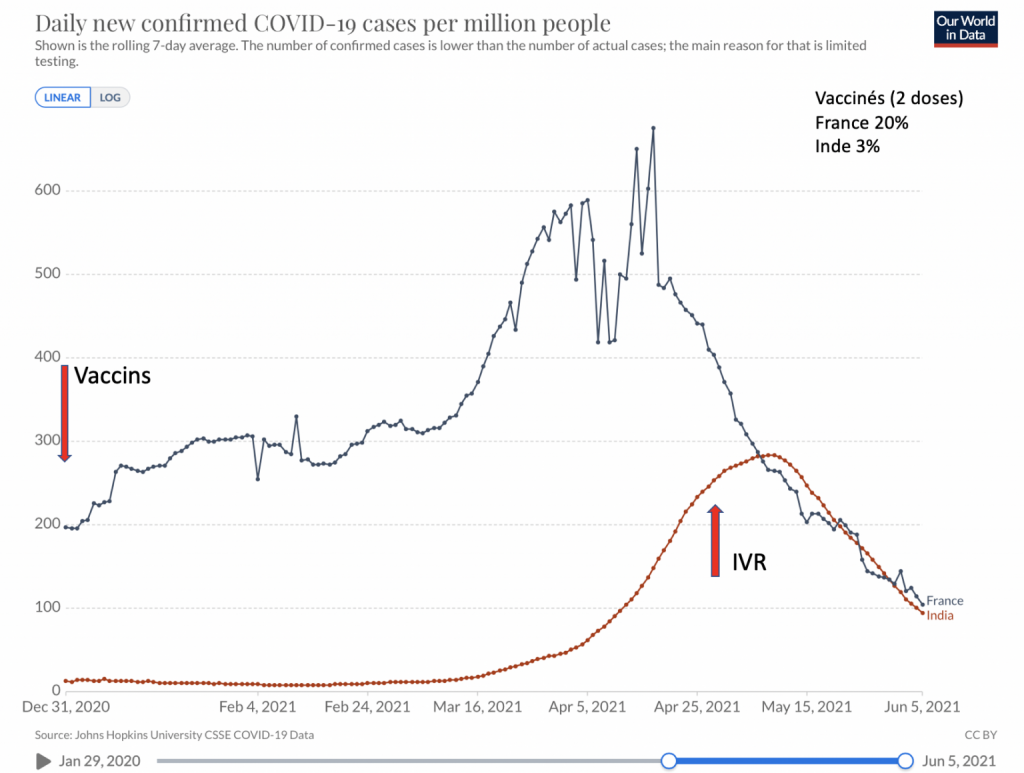
The figures are from Johns Hopkins University, they are the daily figures averaged over 7 days to avoid weekend breaks. These figures are reported per million inhabitants, to compare 2 countries with unequal populations. We can also see that the Indian wave, as I said since the first day, is much lower in intensity than what France was experiencing. We also see that ivermectin worked well on the Indian variant. Finally, some will tell you that the Indian figures are understated; if this is the case, it is of no importance here to follow an evolution over several months, the collection conditions being the same over the entire period. “
Apparently ivermectin costs the state 10 euros for 15 kilos of the medicine. The daily dose per person depends on their weight – 0.2 milligrams per kilo. Which would, for someone weighing 80 kilos, cost the state (admittedly before packaging etc.) just 1.6 euros for 10,000 days’ supply (or, more rationally, less than half a cent for 30 days’ supply or, even more logically since the disease can be cured in considerably less than 30 days, 0.16 cents for 10 days) . Ivermectin was discovered and developed by Satoshi Omurai who received a Nobel prize for it in 2015.
Interesting discussion between American evolutionary biologist and American doctor about current situation, ivermectin (and its history) and the vaccines
This video stayed up for a few days until Youtube decided it violated their Big Brother “community guidelines”. But there’s a podcast downloadable podcast version here
Sample quote:
Doctor: “There were four patients. We knew they were clotting to degrees that we hadn’t seen and there was so much controversy around putting someone on a blood thinner…people are put on blood thinners in hospitals for far less resons than we were promoting with this and so it was just evidence-based maniacism…bizarre…You can’t observe, you can’t make clinical reasoning, you can’t deduce, you need a trial before you do anything”
Biologist: “This is exactly the same in my field. People who are really good at evolutionary biology or ecologists…have intuition, they know how to follow a hunch, they know how to figure out when their hunches are wrong…The point is it’s an art more than a science actually and in the case of a brand-new pandemic that is spreading like wildfire this is of course exactly the mindset that you want. You want people who are capable of figuring out if there is some pattern and then deduce whether they were fooled by some sort of noise-pattern or whether it was actually something, testing a hypothesis but there is a point at which you know and you know better than a study because you’ve acted on that hunch and you’ve seen patients get better and it happens enough times that it can’t be random…Anyway, there’s something about the mindset of the moment – it’s all about peer review…and it’s all about the official guidance from the W.H.O. and the CDC [Centers for Disease Control and Prevention] and it’s basically a kind of intellectual authoritarianism that is so bizarre in the context of a complex system like medicine especially in the context of a brand-new disease that we’re all not experts in. There are no experts that we can simply default to. Everybody’s anomalous.”
Doctor: “I like that term ‘intellectual authoritarianism’. I don’t know if it was occurring to that degree or remotely to that degree pre-Covid…I started to see all the institutions coming out with their treatment protocols – you weren’t allowed to stray from the protocol…suddenly I felt like I was being handcuffed…it was bizarre – I’ve never seen that in my life before.”
Biologist: “I have the sense that doctors have been demoted – forcibly demoted – from the position of scientific clinician to technician and the point is you’re really delivering a pre-packaged good more than you are coming to understand your patient and what they therefore need – and it’s a travesty.”
Doctor: “I’ve never been asked to do that before. I’ve always been asked to use to the best extent my experience, my judgement and insight to best help the patient. That’s the oath I took. The oath wasn’t “Do what the Gods of Science and Knowledge say.”. We’ just little mortals and we have to listen to the Gods. I’ve never been asked that before…Many of them are just desk jockeys – I mean they’re not on the frontlines. They’re reading some papers, they think they know what the disease is, they don’t know what the disease is, they’re not sweating it out, seeing day-to-day the manifestations, the responses to therapy, the lack of responses, they don’t understand this disease and yet they’re telling everyone how to treat it. We want a seat the table, expert clinicians – where’s the expert clinician committee?”
This is illustrative of the developing proletarianisation of the medical middle class , with all the contradictions of its middle class complaints and angst, which are very valid whilst at the same time also failing to recognise how this proletarianisation is, and has long been, replicated amongst those who are lower in the hierarchy, even if often very different ways. Of course, one must add that this is not proletarianisation in any financial sense, at least as yet, nor probably in the forseeable future.
More on ivermectin
“Michael Capuzzo, a New York Times best-selling author , has just published an article titled “The Drug That Cracked Covid”. The 15-page article chronicles the gargantuan struggle being waged by frontline doctors on all continents to get ivermectin approved as a Covid-19 treatment, as well as the tireless efforts by reporters, media outlets and social media companies to thwart them. Because of ivermectin, Capuzzo says, there are “hundreds of thousands, actually millions, of people around the world, from Uttar Pradesh in India to Peru to Brazil, who are living and not dying.” Yet media outlets have done all they can to “debunk” the notion that ivermectin may serve as an effective, easily accessible and affordable treatment for Covid-19. They have parroted the arguments laid out by health regulators around the world that there just isn’t enough evidence to justify its use. For his part, Capuzzo, as a reporter, “saw with [his] own eyes the other side [of the story]” that has gone unreported, of the many patients in the US whose lives have been saved by ivermectin and of five of the doctors that have led the battle to save lives around the world, Paul Marik, Umberto Meduri, José Iglesias, Pierre Kory and Joe Varon. These are all highly decorated doctors. Through their leadership of the Front Line COVID-19 Critical Care (FLCCC) Alliance, they have already enhanced our treatment of Covid-19 by discovering and promoting the use of Corticoid steroids against the virus. But their calls for ivermectin to also be used have met with a wall of resistance from healthcare regulators and a wall of silence from media outlets…On December 8 2020, FLCCC member Dr Pierre Kory gave nine minutes of impassioned testimony to the US Homeland Security Committee Meeting on the potent anti-viral, anti-inflammatory benefits of ivermectin. A total of 9 million people (myself included) saw the video on YouTube before it was taken down by YouTube’s owner, Google. As Capuzzo exhaustively lays out, both traditional and social media have gone to extraordinary lengths to keep people in the dark about ivermectin. So effective has this been that even in some of the countries that have benefited most from its use (such as Mexico and Argentina) many people are completely unaware of its existence.”
Discussion of trials and meta-analyses of ivermectin
“…Somehow at the root of all this is some weird license with no limit to a double standard. So if the powers-that-be decide they don’t like something like ivermectin they can establish any standard up to a ridiculous degree that nothing can overcome. When it comes to the thing that they favor there’s almost no standard at all. There’s no level of danger that could be sufficient to call it into question…What you can see is a double standard that is glaring if you know how to analyse what’s being said…In light of conspicuous patterns…and in the light of the first that the drug in question has a very long extreme safety record why wouldn’t you test it, why wouldn’t you do that large scale study, why wouldn’t you deploy it somewhere to see whether it had the effect and then discover whether or not this was…effective in controlling Covid from people who’ve already contracted it and preventing contraction…What on earth is the excuse for not testing this…remarkable efficacy short term and long term – because it’s been in use so long. Given all the evidence this appears efficacious in preventing both the spread between people and the spread within a person, why on earth would you not run a very large study that would tell you for sure how good this was and how best to use it…If ivermectin were an effective treatment, the vaccines would never have gotten emergency use authorisation in the U.S. and we know that because [cites official document listing “Criteria for issuance under emergency use authorisation of medical products”]... It needs to be a serious or life-threatening disease or condition. There needs to be evidence of effectiveness. There needs to a be a risk/benefit analysis. And there need to be no alternatives. Quote: “For the FDA to issue an EUA, there must be no adequate, approved and available alternative to the candidate product for diagnosing, preventing or treating the disease or condition”…By not doing the relevant large-scale clinical studies on ivermectin and thus it not being approved by the FDA for use in Covid that opens the door for …emergency use authorisation for the vaccines that we are now all living with and among…This would have elements of malpractice, this would be gross negligence…and it verges on depraved indifference…”
Ivermectin is a vastly cheaper method of treating Covid than the vaccines. Apparently ivermectin costs the state 10 euros for 15 kilos of the medicine. The daily dose per person depends on their weight – 0.2 milligrams per kilo. Which would, for someone weighing 80 kilos, cost the state (admittedly before packaging, delivery costs, etc.) just 1.6 euros for 10,000 days’ supply (or, more rationally, less than half a cent for 30 days’ supply, or even more rationally – since you’re likely to recover after less than 10 days, 0.16 of a centime for 10 days).
Dr Sebastian Rushworth looks at the trials of ivermectin
“You would have thought that this strong overall signal of benefit in the midst of a pandemic would have mobilized the powers that be to arrange multiple large randomized trials to confirm these results as quickly as possible, and that the major medical journals would be falling over each other to be the first to publish these studies.
That hasn’t happened.
Rather the opposite, in fact. South Africa has even gone so far as to ban doctors from using ivermectin on covid-19 patients. And as far as I can tell, most of the discussion about ivermectin in mainstream media (and in the medical press) has centred not around its relative merits, but more around how its proponents are clearly deluded tin foil hat wearing crazies who are using social media to manipulate the masses.”
See also this, from the same doctor, which concludes that hydroxychloroquine with azythromicine and zinc might be a bit beneficial but probably not much, although he feels the most reliable trials involve too few people to be sufficiently conclusive. Includes both in the article itself and in the comments boxes an interesting debate about how research with placebos and double blinds often cherry-picks and manipulates data, depending on things such as the age and comorbidities of those selected, the time-gap following the onset of symptoms when treatment is given, the doses involved, the effect measured and details of the measurement, distribution of SARS-CoV-2 variants, and other treatments (anything from supplements, other medications, or other kinds of treatment like prone positioning).
Sample quote: “RCTs [randomised control trials] are considered the gold standard by corporations and academics who most benefit by them, whereas anecdotal reports based on clinical experience are ignored. In theory RCTs sound good and they do have some utility wiping out the obvious confounders of the worthless correlation studies. That does not mean they are of ultimate value – it merely points to how worthless the observational studies are. RCTs only appear good in relative comparison, but you’re comparing dumb and dumber, not right and wrong. … Note that pharma can fund an RCT, and if it does not make their new multi-million dollar drug look good, they throw it out and start a new RCT with different parameters. No one, including MDs, knows what the prior RCTs concluded. Research form Harvard’s Safra Center found that 90% of new pharma drugs did next to nothing (except give Pharma big profit) – they provided maybe a 2% improvement (probably jiggered to pass the FDA rubber-stamp approval threshold (Pharma funds half the FDA’s budget and staffs it via the revolving door). We live in a post-truth world where we are programmed from every direction. It is not easy to think for yourself since we’ve been programmed from birth with unexamined assumptions. Science (including lots of anecdotal reports) is our only hope to do an end-run around our internal confirmation and availability bases as well as both the mainstream and alt-programming. You can’t really trust anyone and can’t trust RCTs either. It’s not easy moving onward through the fog and you have to be ready to backtrack so no ego allowed. You have to do your own research and Hope for the Best. As Socrates pointed out, realizing your own ignorance (as well as that of others) is the beginning of wisdom. “It Ain’t What You Don’t Know That Gets You Into Trouble. It’s What You Know for Sure That Just Ain’t So.” – Twain”
The victories of ivermictin
Translation:
“You can fool some of the people all the time. You can fool all the people some of the time. But you can’t fool all the people all the time.” (A. Lincoln)
Ivermectin has already saved tens of thousands of lives, and is gaining ground. The problem is that the pharmaceutical industry, the western governments, don’t want to see it, and the press refuses to show it to us. It is making progress, but how many tens, hundreds of thousands of lives have been lost in one year because of this blindness? If ivermectin cures river blindness, it seems to be a failure against Covid blindness.
INDIA
By mid 2020, Uttar Pradesh in India was the first “country” (actually a state in India but with a population of 205 million, 3 times the size of France) to treat its population extensively with Ivermectin. Chiapas in Mexico did the same at about the same time.
In 2020, Uttar Pradesh had 7,800 deaths, compared to 65,000 here, which is 25 times less than us for the same population. A younger population, you may say, but the health conditions are much poorer, as we see today. Not all declared? Not to that extent! So to be fairer, let’s compare with another Indian state, like Delhi, which is 12 times less, and 3 times less than the country’s average. Same thing for Chiapas: with ivermectin, 4 times less deaths than the country average, 10 times less than Mexico City.
No one in the West was interested. Instead of seeing what was happening on a large scale, our authorities were quibbling about 2×12 studies, wondering whether they were published or not, whether the authors thought a few more guinea pigs were needed, without even looking at the results. Foolishness? Incompetence? Manipulation? I leave it to you to judge.
While 15 days ago everyone was talking about a catastrophe in India, a situation out of control, knowing that they had to deal with their second wave, I took the opposite view and calmed things down.
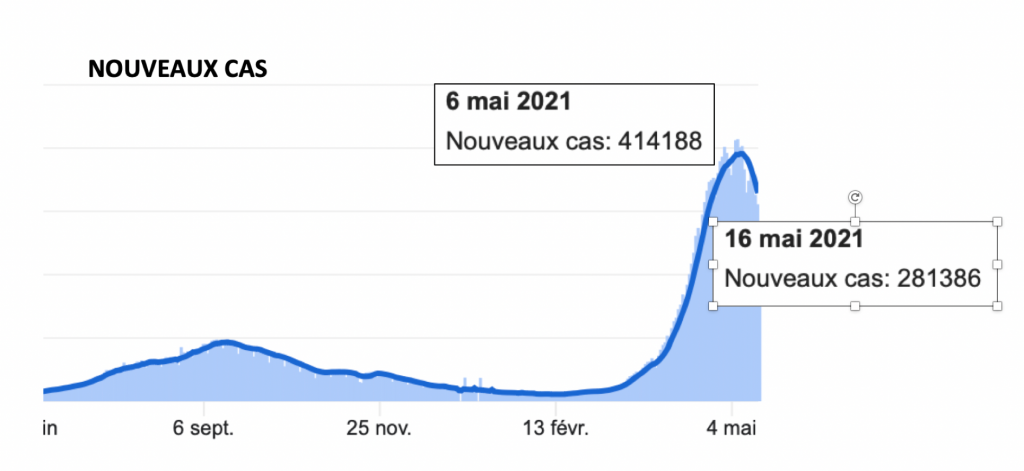
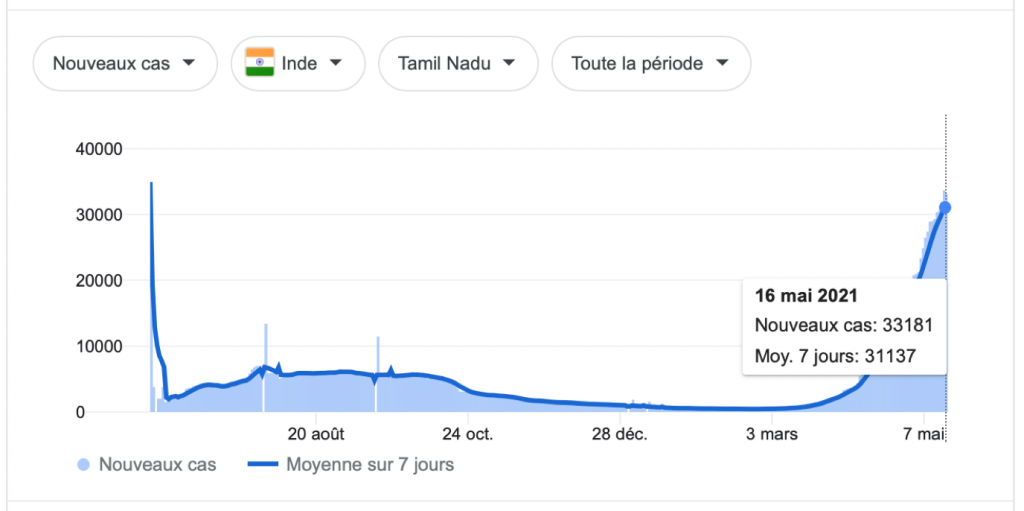
What about after 2 weeks? While our “great specialists” were still announcing a few days ago that India would not reach its peak of contamination before several weeks (repeated everywhere like here), here is the curve of the contaminations in India, up to date yesterday: it is eight days since the peak seems to have been reached.
How is this possible, so quickly, in a country where barely 3% of the population has had its two doses of vaccine so far? Many states have followed Uttar Pardesh. Goa followed (in 15 days reduction of 58% in hospitalisations), asking the whole population to take Ivermectin, then Uttarakhand and others.
What do the curves look like in these states?
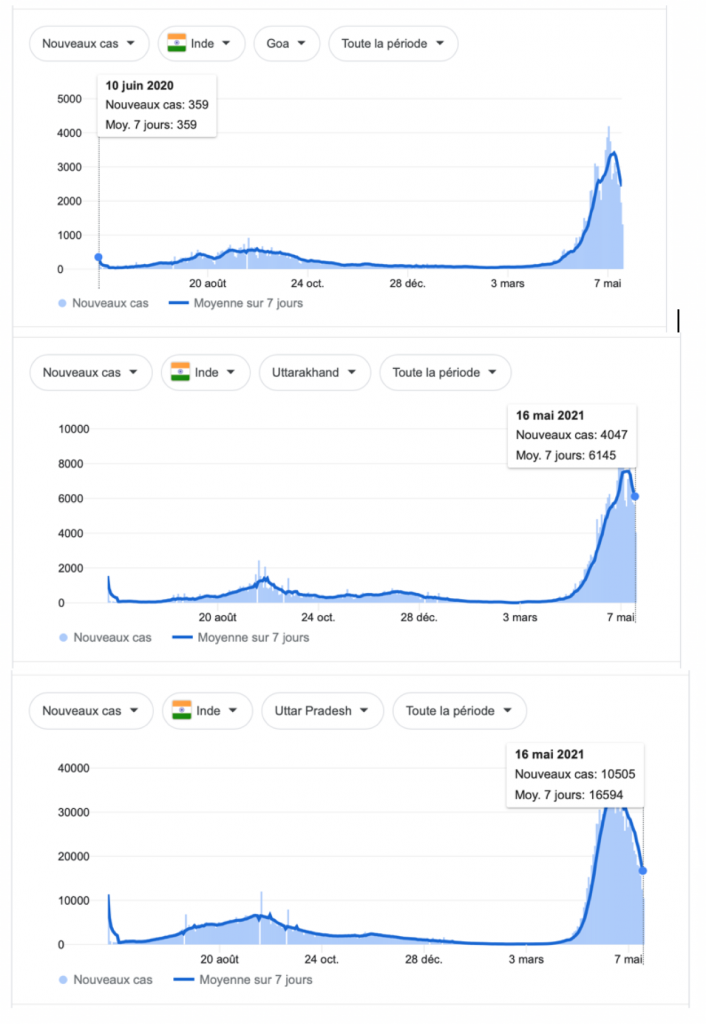
But WHO and Big Pharma are watching. The WHO issued statements advising against Ivermectin, and Gilead showered the country with Remdesivir, even though it was advised against by the WHO, at a 20-fold price reduction. Some states followed the WHO, such as Tamil Nadu. Here is what it looks like: no decline. If you want all these curves day by day, type on Google “Covid India”, and you immediately have the curves of cases and deaths for all countries. For India, just to the right of the country, you can select each state. You can also find other curves on Patrice Gibertie’s website.
As far as deaths are concerned, given the 15-day lag with cases, when we were at 3000/day, I thought the peak would be between 5 and 6,000, it will be less because it seems to have plateaued at around 4,000 for the last week.
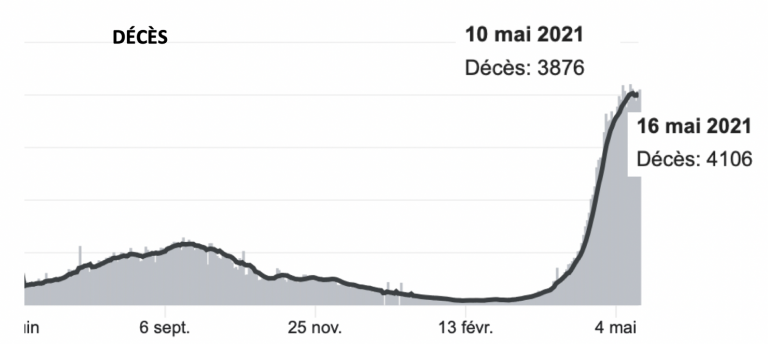
If this continues, the peak of the Indian “catastrophe” is at the level of what we have been experiencing on average for the last 6 months, and will have lasted only 10 days. Let’s remember that we had a peak of 1000 deaths in 24 hours, that is to say 20,000 in relation to their population. Having said that, let’s remember that with this virus, everything can change from one day to the next, but it seems to have taken hold in the last 8 days.
MEXICO
Same thing in Mexico. Following the results of Chiapas, Mexico City has started to distribute Ivermectin on a large scale. Who told us about the results of this experiment, involving 234,000 patients, with a 2/3 reduction in hospitalisations? Nobody.
This country was remarkably followed by Enzo Lolo.
OTHER
Other countries have started using Ivermectin, but the results will not necessarily be seen. So when the Czech Republic announced it, and at the same time ordered 20,000 doses for the whole country, there is a gap between talk and practice.
Portugal does not make any noise, doctors are free and prescribe a lot (50% it seems). All this, unlike in France, with the agreement of the Order of Physicians. Result:

South Africa has also started, under pressure from doctors’ associations:

I was the first in France to tell you the story of Ivermectin in this country, which was banned and abruptly authorised after members of the government died, while others were still living thanks to Ivermectin and Jackie Stone.

One of the latest countries is the Philippines, and as always, cases fall within 15 days:

FRANCE
By way of comparison, the curve for France, which is not treating and is struggling to get over its second wave, which will have lasted more than 6 months. The declarations of satisfaction of our leaders are increasingly difficult to find comparisons to continue to say that we are better than the others.
CONCLUSIONS
It would seem that to stop a wave, ivermectin alone (less than 3% of those vaccinated with 2 doses in India, 1.5% in Zimbabwe, 1% in South Africa), goes much faster than vaccines alone. 15 days for the first, several months for the other. Also our vaccines seem to have problems with the Indian variant, whereas ivemectin does not.
Not treating Covid in its early stages is like an oncologist waiting for metastases before starting cancer treatment, like a surgeon waiting for sepsis and peritonitis before operating on appendicitis. This is the medicine we practice today.
SF: see also Ivermectin and this from the end of May (in French – rough translation here)
Ivermictin subject to arbitrary suppression
“…Social networks are not to be outdone and are participating in this desire to hide the truth about ivermectin. See this impressive regulation of YouTube on this subject. It goes beyond censorship! It is “forbidden to contradict information from local health authorities or the WHO”, “it is forbidden to recommend the use of ivermectin, to say that it is an effective treatment”…”
On ivermictin see also this.
Portuguese doctors supporting use of ivermictin for early treatment of Covid
Translation of doctor’s article on benefits of Ivermectin as compared with the vaccine
Interesting interview in French with dissident doctor
This doctor was for 20 years president of the “Caisse autonome de retraite des medicins de la France” (Autonomous retirement fund for physicians in France). He begins by saying the government has only recommended anti-coagulants and antibiotics and goes on to talk about a doctor who has treated 850 symptomatic Covid patients with azythromycine. Of these 850 patients 2 were hospitalised and nobody died. The French state remains silent about azythromycine and ivermictin. Andrew Hill, who has studied ivermictin says “there was a 75% reduction in mortality” with its use, and apparently it reduces symptoms twice as rapidly as without its use. The study covered 2282 patients. India has distributed 150 million doses of ivermictin and has proportionately 3 times less deaths than France. Ivermictin is forbidden throughout Mexico apart from Chiapas, which has proportionately 4 times less deaths than the other states of the country. On top of all this, the doctor says that GPs throughout France have received an order from the government not allowing them to give sick notes to those who have Covid! Apparently, if people need sick notes they either do it themselves over the internet or they go to hospital. The government doesn’t want them to see their GPs for fear that they may give them azythromicine or ivermectin rather than paracetomol which the government recommends (paracetomol is not something one should take if one has a fever as it suppresses symptoms but also suppresses the body’s capacity to fight the virus). Prescription of ivermectin for Covid has been forbidden since the end of December, but they possibly fear that doctors may prescribe it claiming that the patient has another illness even if the patient has Covid.
https://www.youtube.com/watch?v=cevj37rDRGo
Amongst other things, this says that in France the 3 professors who are the mainstay of televised scientific debates on Covid, TV’s main propagators of vaccines and of opposition to HCQ and Ivermectin, respectively receive 130,000 euros, 170,000 euros and 540,000 euros from the pharmaceutical labs and especially from Gilead, the lab that produced remdesivir, the drug that was dismissed as useless (and possibly dangerous) by the WHO back in November, after a billion euros had been paid to the company by the EU, a drug still used in the UK at least up until mid-December. Gilead also provided the money for the majority of other trials of HCQ, invariably saying it was useless.
Leave a Reply to Sam FantoSamotnaf Cancel reply